Guest Skeptic #1: Dr. Chris Carpenter is Professor of Emergency Medicine at Washington University in St. Louis and a member of their Emergency Medicine Research Core. He is a member of the SAEM Board of Directors and the former Chair of the SAEM EBM Interest Group and ACEP Geriatric Section. He is Deputy Editor-in-Chief of Academic Emergency Medicine. He is also Associate Editor of Annals of Internal Medicine’s ACP Journal Club and the Journal of the American Geriatrics Society, and he serves on the American College of Emergency Physician’s (ACEP) Clinical Policy Committee. Dr. Carpenter also wrote the book on diagnostic testing and clinical decision rules.
Reference: Musey et al. Guidelines for reasonable and appropriate care in the emergency department (GRACE): Recurrent, low-risk chest pain in the emergency department. AEM July 2021
This is an extra special SGEM. It is a combo of an SGEM Xtra and an SGEMHOP. The Society of Academic Emergency Medicine (SAEM) has decided to publish its own clinical practice guidelines (CPGs). They are called Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE). This episode will review the GRACE-1 guideline looking at low-risk recurrent chest pain.
Because this is a new initiative by SAEM, I interviewed Dr. Chris Carpenter about these new GRACE guidelines.

Dr. Chris Carpenter
Listen to the SGEM podcast to hear him answer five background questions about these new CPGs.
- Who came up with the idea of doing CPGs?
- Why do we need more guidelines?
- Walk us through the GRACE process?
- Why pick recurrent, low-risk chest pain to be the first CPG?
- What do you hope to achieve with these CPGs
Guest Skeptic #2: Dr. Suneel Upadhye is an Associate Professor of Emergency Medicine & Clinical Epidemiology at McMaster University. He is a founding member of the Best Evidence in Emergency Medicine (BEEM) program. Suneel is also the inaugural Research Lead for the EM Researchers of Niagara, which is a novel community-based EM research group within Niagara region, Canada. He is also a Guidelines Methodologist within CAEP and the SAEM GRACE groups.
Case: You are seeing a patient who has returned to the emergency department (ED) with recurrent chest pain. It is their fourth visit in the last twelve months. He has had his chest pain for approximately three to four hours now and is not classic for ischemic symptomatology. His initial high-sensitivity (hs) troponin is negative, and his ECG is unremarkable. In reviewing his records, you note that he has undergone significant cardiac testing in the recent past, which was unremarkable. This included a normal exercise stress test and CCTA 18 months ago. You also note that he has an underlying anxiety disorder, which is being treated and followed by his family physician.
Background: This new SAEM GRACE initiative is committed to using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system, GRADE was pioneered at McMaster University, in creating rigorous, transparent, and trustworthy guidelines on common clinical problems for emergency medicine (EM) physicians that are not always directly studied in EM research activities.
The steering group/panelists explored many different potential questions, and voted on the top eight, that were then reviewed in systematic fashion; evidence was rated using GRADE methods, and then final recommendations were made using the GRADE Evidence-to-Decision framework (Upadhye et al CJEM 2021 and Courtney and Lang AEM 2021). The Methods team sought initial GRADE training, then shared that learned expertise with the question groups, many of whom were relative novices in guideline methodology.
After two years, a comprehensive document is being published that answers the key diagnostic dilemmas in recurrent chest pain patients who have had recent normal cardiac investigations, to streamline testing and ED length of stay without risk of major adverse coronary events (MACE) at 30 days.
CLINICAL QUESTION: WHAT ARE THE RECOMMENDATIONS FOR MANAGING PATIENTS WITH RECURRENT, LOW-RISK CHEST PAIN IN THE ED?
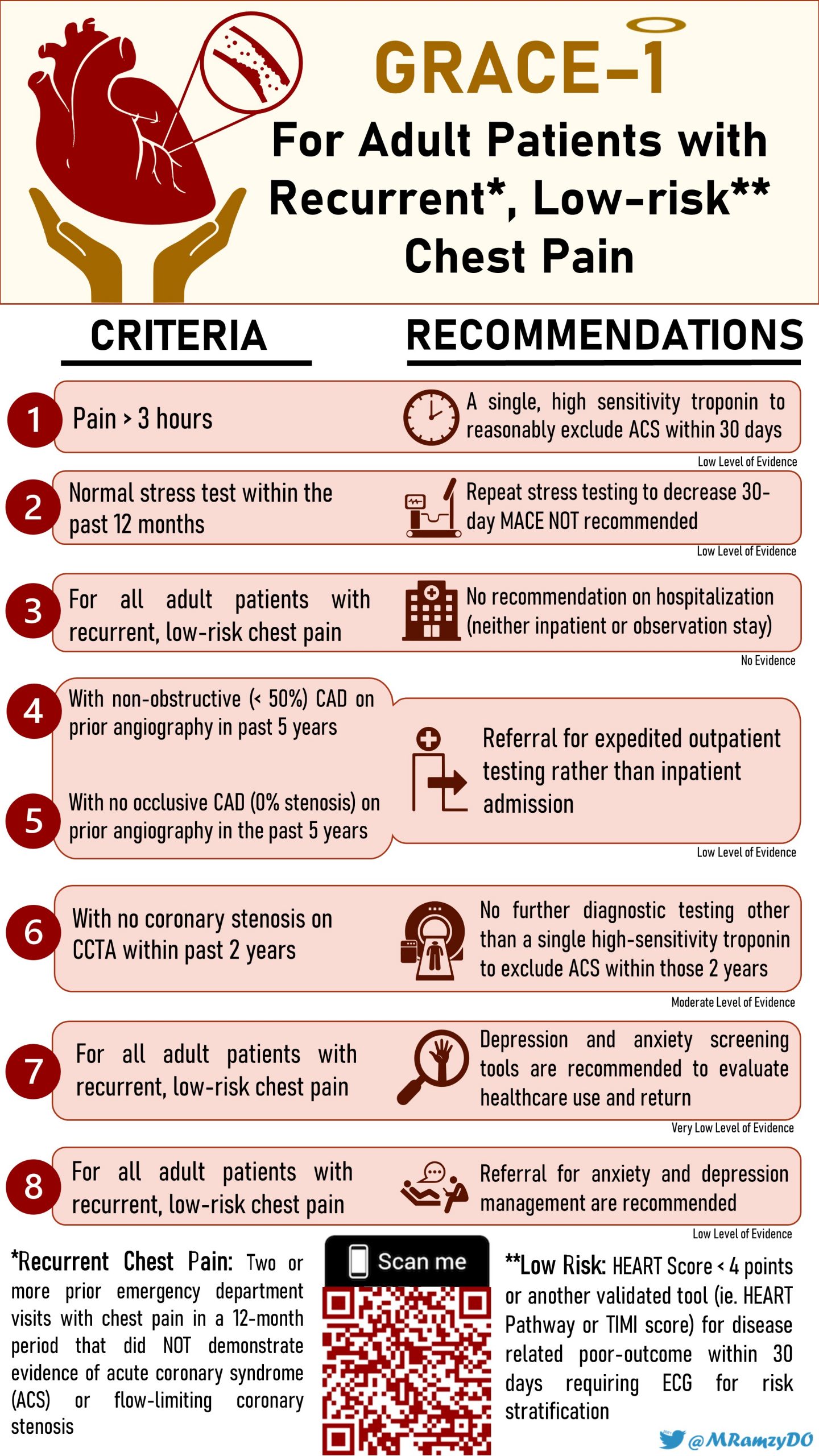
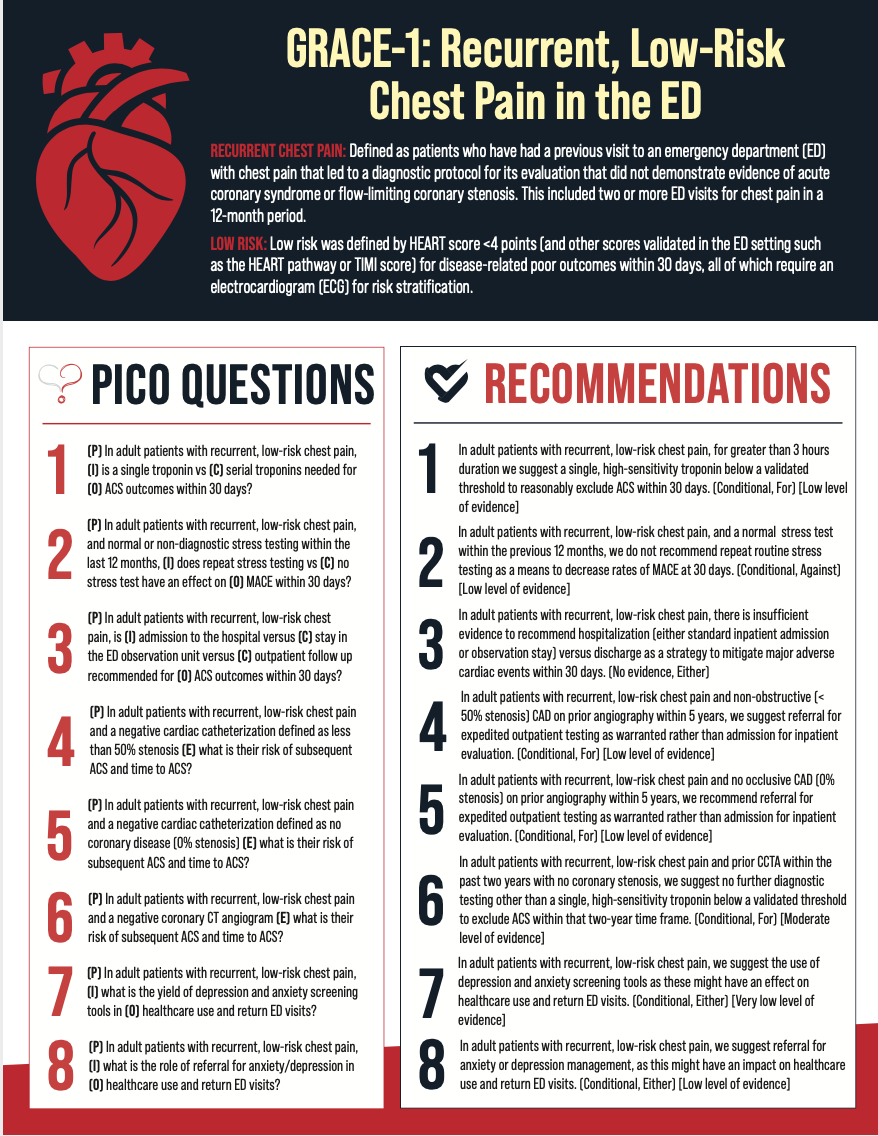
- Recurrent Chest Pain: Patients who have had a previous visit to an ED with chest pain that led to a diagnostic protocol for its evaluation that did not demonstrate evidence of acute coronary syndrome (ACS) or flow-limiting coronary stenosis. This included two or more ED visits for chest pain in a 12-month period.
- Low-Risk: This was defined by HEART score <4 points (and other scores validated in the ED setting such as the HEART pathway or TIMI score) for disease-related poor outcomes within 30 days all of which require an electrocardiogram (ECG) for risk stratification.
- Expedited: This was considered a period of three to five days.
There is no 100% guaranteed safety outcome for patients with low-risk chest pain with respect to 30-day MACE, but the “warranty” on negative high-sensitivity troponin test results (assay- and institution-dependent), either single or double tests “x” hours apart, should be reassuring to ED physicians to discharge such patients with reasonably expedited follow-up.
This 30-day MACE risk is even lower when there is a negative CCTA result (ie. no coronary stenosis) in the preceding two years, or less than 50% obstructing stenosis on prior angiography in preceding five years. Finally, in patients in whom depression/anxiety might be a driver of recurrent ED visits for low-risk chest pain, use of screening tools in the ED for mood disorder detection and subsequent referral for mental health supports may be warranted.
Reference: Musey et al. Guidelines for reasonable and appropriate care in the emergency department (GRACE): Recurrent, low-risk chest pain in the emergency department. AEM July 2021
Authors’ Conclusions: “These guidelines outline and summarize the evidence and strength of GRACE recommendations regarding eight priority questions of interest to emergency clinicians, other healthcare professionals, patients, and policymakers with regard to the evaluation and management of patients with recurrent, low-risk chest pain seen in the ED. Direct evidence for the selected priority questions in this population is lacking, which highlights areas which will benefit from further robust prospective investigation in this specific population.”
 Quality Checklist for a Diagnostic Study:
Quality Checklist for a Diagnostic Study:
- The study population included or focused on those in the emergency department? Yes
- An explicit and sensible process was used to identify, select and combine evidence? Yes
- The quality of the evidence was explicitly assessed using a validated instrument? Unsure
- An explicit and sensible process was used to the relative value of different outcomes? Unsure
- The guideline thoughtfully balances desirable and undesirable effects? Yes
- The guideline accounts for important recent developments? Yes
- The guidelines has been peer-reviewed and tested? Yes/No
- Practical, actionable and clinically important recommendations are made? Yes
- The guideline authors’ conflicts of interest are fully reported, transparent and unlikely to sway the recommendations of the guidelines? Yes
GRACE-1 RECOMMENDATIONS: