
Podcast: Play in new window | Download
“This learning material is sourced from Emergency Medicine Cases and has been published here with permission as per creative commons copyright”
Drug interaction-related morbidity and mortality is highly under-recognized in Emergency Medicine. Patients who present with altered level of awareness, delirium, syncope and falls are often admitted to hospital without a definitive diagnosis; and only later is it recognized that a drug interaction was at play. Thirty percent of ED patients have at least one drug related problem contributing to their ED visit, which includes adverse drug reactions and subtherapeutic dosing. More than 1 in 9 ED visits are due to drug related adverse events, and many of these drug-related adverse events are due to drug interactions which are almost entirely preventable. In this EM Cases podcast Dr. David Juulink, Dr. Walter Himmel and Anton delve into some common presentations that require having drug interactions in the differential diagnosis, which combinations of drugs to avoid when ordering in the ED and when prescribing for outpatient therapy from the ED, high risk patients for drug interactions and the top 3 drug categories to be aware of when it comes to drug interactions…
Podcast production, sound design & editing by Anton Helman
Written Summary and blog post by Kate Dillon and Ian Beamish,
edited by Anton Helman June, 2023
Cite this podcast as: Helman, A. Himmel, W. Juurlink, D. Must Know Drug Interactions in Emergency Medicine. Emergency Medicine Cases. June, 2023. https://emergencymedicinecases.com/drug-interactions-emergency-medicine. Accessed July 2, 2023
First, we need to understand the difference between pharmacokinetics and pharmacodynamics
All drug interactions can be split into pharmacokinetic and pharmacodynamic interactions.
Pharmacokinetics can be thought of simply as what a body does to the drug. Drugs are absorbed, distributed, metabolized, and excreted. Anything that disturbs these processes can change the serum drug level.
Pharmacodynamics can be thought of simply as the effect of the drug on the body. For example, the synergistic impact that two drugs might have on prolonging the QT interval.
When to consider drug interactions in the differential diagnosis
It is easy to say that drug interactions should always be considered in any ED presentation, but this approach is not practical. Although many clinical scenarios could theoretically be explained by drug-drug interactions, some of the ones that we should be particularly wary of, especially if patients are on multiple medications, or have recently had a change/addition of a new medication are:
- Syncope/near-Syncope
- Delirium/altered LOA
- Falls
- Any unexplained clinical presentation after initial ED workup
Who are high risk patients for drug interactions, and why are they high risk?
1.Older Patients are at high risk for drug interactions
Fifteen percent of older patients have adverse drug reactions and 50% of these are preventable. Some of the reasons behind this are that they often are taking more drugs than younger people, they often have comorbidities like renal dysfunction that make drug interactions more likely, if they have cognitive dysfunction they may be more likely to manifest drug-drug interactions, and they are more frail, making them less able to tolerate drug interactions.
Drugs that are higher risk for interactions in older patients include:
- Drugs that have a narrow therapeutic range including anticoagulants, hypoglycemic agents (sulfonylureas, insulin), digoxin, sedatives, immunosuppressants and anticonvulsants
- Antibiotics
- Analgesics including NSAIDs and opioids
2.Patients on psychiatric medications are at high risk for drug interactions
Psychiatric medications can impact multiple systems/receptors and can have additive effects when combined causing serotonin syndrome, neuroleptic malignant syndrome,
Serotonin syndrome
Antidepressants often act on the serotonin system, and in combination, at high doses, and with other medications (antipsychotics, lithium, fentanyl, cocaine, methadone, metoclopramide etc.) can increase the risk of developing serotonin syndrome. Although classic presentations with a constellation of hyperthermia, hypertension, tachycardia, altered mental status, diaphoresis, clonus/hyperreflexia, agitation, and seizures can occur, they can also be more subtle and should be on our differential in patients who are on serotonergic agents.
Clinical pearl: there are case reports of inducing serotonin syndrome in patients taking SSRIs who are given fentanyl during procedural sedation in the ED. In patients receiving this combination of drugs who are agitated post-sedation, consider serotonin syndrome on your differential diagnosis.
Neuroleptic malignant syndrome
Antipsychotics in combination, at regular doses or at high doses can increase the risk of neuroleptic malignant syndrome (NMS) causing autonomic instability.
NMS Diagnostic Criteria: two of the following: fever, muscle rigidity, tachycardia, altered mental status, high BP, excessive sweating.
Clinical Pearl: The key distinguishing features between NMS compared to serotonin syndrome are that patients with NMS often have lead pipe muscle rigidity while patients with serotonin syndrome often have clonus and/or hyperreflexia. Simply checking the tone and reflexes can clinch these diagnoses.
CNS depression
Many of the psychiatric medications that are prescribed have sedative effects, and the additive effects of these medications (especially if combined with other substances like alcohol or opiates) can have profound impacts on patient’s cognitive function.
QT Prolongation
There are many medications, including psychiatric medications, that can lead to QT prolongation. An up-to-date list of medications can be found at crediblemeds.org. The impact on the QT interval depends not only on the number of drugs and what classes of drugs that a patient is taking, but the specific medications within these classes (given intraclass differences in the risk for QT prolongation). Some of the more commonly used higher risk medications include citalopram, escitalopram, ondansetron and moxifloxacin. Consider a screening ECG for patients who are already on QT prolonging drugs if you are considering adding another one.
Intraclass Differences in QT Prolongation
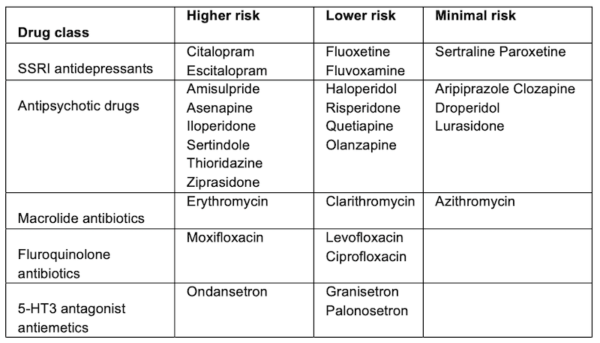
Clinical Pearl: think of the “antis” when considering QT prolongation (i.e., antiemetics, antidepressants, antipsychotics, antiemetics, antibiotics).
3.Renal patients are at high risk for drug interactions
Patients with renal dysfunction are at higher risk for drug interactions due to a combination of impaired clearance of drugs, as well as the greater number of medications that these patients are on to treat the conditions that contribute to their renal dysfunction (i.e., diabetes, HTN, atherosclerosis).
There are three specific scenarios we should be aware of when thinking of drug-interactions in patients with renal dysfunction:
1.Hyperkalemia: kidneys are critical for getting rid of potassium, and if the GFR is reduced, then patients will be at higher risk of developing hyperkalemia. There are many drugs that can pre-dispose to hyperkalemia, including ACE inhibitors, ARBs, spironolactone, trimethoprim-sulfamethoxazole (TMP-SMX – Septra/Bactrim), heparin and NSAIDs. The risk of hyperkalemia increases when these medications are combined in patients with decreased ability to eliminate potassium.
TMP-SMX (Septra or Bactrim) deserves special attention for drug interactions causing hyperkalemia:
- Trimethoprim and spironolactone taken together increase the risk for hyperkalemia with a clear association between trimethoprim and sudden cardiac death
- There is a 12 fold increased risk in hospital admission for hyperkalemia in elderly patients taking trimethoprim in combination with spironolactone compared to amoxicillin in combination with spironolactone
- There is a 7 fold increased risk in hospital admission for hyperkalemia in elderly patients taking trimethoprim in combination with ACE inhibitors or ARBs compared to amoxicillin in combination with ACE inhibitors or ARBs
EM Quick Hit with Dr. Juurlink on TMP-SMX related interactions
2.Impaired drug elimination: drugs we should remember to dose- or interval-adjust for renal dysfunction include DOACs, digoxin and colchicine.
3.Phosphate binders: patients with advanced renal disease will often be on a phosphate binder like calcium carbonate. Calcium, as well as iron and magnesium can form complexes with other medications in the lumen of the GI tract and inhibit their absorption. Medications that are particularly susceptible are quinolones, tetracyclines and levothyroxine. Patients should be advised to take these medications at different times of day to limit these interactions.
Essential categories of drugs for drug interactions in the ED: Antimicrobials, analgesics and cardiovascular drugs
Antimicrobial drug interactions
Antibiotics have a host of potential drug interactions associated with them, especially quinolones, macrolides, and trimethoprim-sulfamethoxazole.
Trimethoprim-Sulfamethoxazole (Septra/Bactrim) interacts with ACEi/ARB, spironolactone, sulfonylureas and warfarin
- ACEi/ARB/Spironolactone + TMX-SMZ -> hyperkalemia (see above)
- Sulfonylurea + TMP-SMX -> hypoglycemia
- Warfarin + TMP-SMX -> supratherapeutic INR and bleeding
Macrolides interact with statins, calcium channel blockers and quinolones
- Clarithromycin, erythromycin + lipophilic statins (think ALS– Atorvastatin, Lovastatin, Simvastatin) -> 10-16-fold increase in the blood concentrations of these statins, increasing the risk for rhabdomyolysis.
- Erythromycin and clarithromycin + amlodipine -> hypotension
Ciprofloxacin + “ALS” statins – > rhabdomyolysis.
Clinical Pearl: of the macrolides, azithromycin is the safest when it comes to drug interactions as it does not inhibit the CYP 3A4 enzyme and has the least impact on the QT interval.
Clinical Pearl: the statins that are higher risk for drug interactions with antibiotics are the “ALS” statins – Atorvastatin, Lovastatin, Simvastatin (especially Simvastatin).
Analgesics drug interactions
Opioids are at high risk for drug interactions related to their impact on the CNS, especially when combined with other sedating medications or substances including benzodiazepines, dimenhydrinate, diphenhydramine or sleep medications. The combination of high dose opioids and benzodiazepines in particular confers an increased risk of death.
Clinical Pitfall: combining high dose opioids and benzodiazepines confers an increased risk of death
Clinical Pitfall: Dimenhydrinate (Gravol), a combination of theophylline and diphenhydramine is effective for motion sickness but evidence is lacking for ED patients with nausea/vomiting. It has potentially dangerous sedative effects that can be worsened when combined with other sedatives (i.e., opioids).
Deep dive into the evidence for anti-emetics: Episode 127 Drugs that Work and Drugs that Don’t
NSAIDs
- Celecoxib + metoprolol -> bradycardia.
- Celecoxib + codeine or tramadol -> decreased analgesic effect (celecoxib inhibits the enzyme that turns the inactive opioid analgesics codeine and tramadol into their active formats. This drug interaction can lead to inadequate analgesic response to these medications.)
- NSAIDs + ASA -> arterial thrombosis (patients who are taking ASA for coronary artery disease – especially if they have a recent coronary stent are thought to be at increased risk for coronary occlusion if NSAIDs are combined with ASA)
Clinical Pitfall: be wary of prescribing NSAIDs in patients who are already taking aspirin in patients who have coronary artery disease, especially with a recent stent.
Clinical Pearl: probably the safest NSAIDs from a drug-interaction and side effect profile are short courses of ibuprofen or naproxen.
Clinical Pitfall: adding celecoxib to codeine or tramadol is likely to decrease the analgesic effect of the codeine/tramadol.
Cardiovascular drug interactions
Anticoagulants (DOAC/Warfarin) + antiplatelet drugs (ASA/clopidogrel) -> bleeding.
Clinical Pitfall: many patients continue take ASA for primary prevention of cardiovascular disease despite evidence suggesting that the bleeding harms outweigh any cardiovascular event benefit. When starting a patient on a DOAC in the ED, for say stroke prevention with atrial fibrillation, strongly consider stopping the ASA if the patient is taking it only for primary prevention.
Warfarin + Acetaminophen -> increased INR/bleeding
EM Quick Hits 4 with Dr. Juurlink on Warfarin and Acetaminophen drug interaction
Beta Blockers/Calcium Channel Blockers +Cholinesterase inhibitors (i.e., rivastigmine/Exelon, donepezil/Aricpet) -> bradycardia.
Insulin + beta blockers -> though there is no direct interaction between these two medications, there is some concern for patients who are prone to hypoglycemia, that beta-blockers can mask the sympathetic symptoms that occur with hypoglycemia and can lead to patients missing the early warning signs.
PPI + diuretics -> hypomagnesemia (the diuretic causes the kidneys to waste magnesium and the PPI turns off the transporter that leads to magnesium absorption in the gut).
Clinical Pearl: to add an extra layer of protection against potentially dangerous drug interactions advise patients go to the same pharmacy for all of their medications so that pharmacists and their drug-interaction checkers act as a second level of protection.







