
Podcast: Play in new window | Download
“This learning material is sourced from Emergency Medicine Cases and has been published
here with permission as per creative commons copyright”
Topics in this EM Quick Hits podcast
Anand Swaminathan on the role of methylene blue in septic shock (0:39)
Nour Khatib on TMJ dislocation reduction techniques (5:51)
Hans Rosenberg on a phenotypic approach to Crohn’s disease emergencies (10:31)
Gil Yehudaiff on evidence based analgesics for renal colic (18:23)
Brit Long on the importance of inhaled steroids for asthma (25:22)
Andrew Petrosoniak on hypocalcemia in bleeding trauma patients (35:23)
Topics in this EM Quick Hits podcast
Anand Swaminathan on the role of methylene blue in septic shock (0:39)
Nour Khatib on TMJ dislocation reduction techniques (5:51)
Hans Rosenberg on a phenotypic approach to Crohn’s disease emergencies (10:31)
Gil Yehudaiff on evidence based analgesics for renal colic (18:23)
Brit Long on the importance of inhaled steroids for asthma (25:22)
Andrew Petrosoniak on hypocalcemia in bleeding trauma patients (35:23)
Podcast production, editing and sound design by Anton Helman
Written summary & blog post by Shaila Gunn, Brit Long, Andrew Petrosoniak, edited by Anton Helman
Cite this podcast as: Helman, A. Swaminathan, A. Khatib, A. Rosenberg, H. Yehudaiff, G. Long, B. Petrosoniak, A. EM Quick Hits 51 – Methylene Blue in Septic Shock, TMJ Dislocation, Crohn’s Disease, Analgesia for Renal Colic, Inhaled Steroids for Asthma, Hypocalcemia in Bleeding Trauma Patients. Emergency Medicine Cases. September, 2023. https://emergencymedicinecases.com/em-quick-hits-september-2023/. Accessed September 12, 2023.
Methylene Blue – a potential adjunct in refractory septic shock
- The first line vasopressor in septic shock, norepinephrine, is associated with risks at high doses and with prolonged use including dysrhythmias, peripheral ischemia, myocardial dysfunction
- Methylene blue may decrease the amount and duration of vasoactive drugs needed in patient with septic shock
- It decreases nitric oxide levels by inhibiting inducible nitric oxide and enzyme soluble guanylate cyclase, which is believed to restore vasoregulation
- The evidence of methylene blue is limited with small studies showing inconsistent evidence in septic shock
A recent study in Critical Care “Early Adjunctive Methylene Blue in Patients with Septic Shock: A single-center, parallel, double blind randomized controlled trial” by Ibarrea-Estrada et al, asked the question: Does methylene blue expedite the discontinuation of pressors in patients with septic shock?
- P: 92 ICU patients, most mechanically ventilated and on norepinephrine and vasopressin
- I: Methylene blue IV infusion 100 mg in 500 cc of 9% normal saline over 6 hours daily x 3 doses
- C: 500 cc of 0.9 % saline
- O: The time to discontinue vasopressors (defined as the discontinuation of all vasopressors for 48 consecutive hours) was 25 hours shorter in the methylene blue group; there was a 1.5 day shorter ICU stay, 2.7 day shorter hospital stay, and a 714 cc lower cumulative fluid balance in the methylene blue group; there was no difference in mechanical ventilation or mortality between groups
Critical Appraisal
- This was a single center trial with a small cohort
- The small cohort is reflective of a selection bias providing limited internal and external validity
- The end-point is not patient centered and may not be clinically relevant
Bottom line => Recent evidence suggests that methylene blue decreases the time spent on vasopressors but does not improve mortality. At this time, the data is not strong enough to recommend the use of methylene blue routinely in vasopressor refractory septic shock, but it can be considered as an adjunct in certain clinical contexts, and our ICU colleagues may be requesting us to administer it, underlying the importance of being familiar with it for this indication.
Atraumatic TMJ dislocations – safe techniques for reduction without sedation
- TMJ dislocations can be atraumatic or traumatic
- Atraumatic jaw dislocations are usually anterior dislocations; this is the most common type of dislocation
- Traumatic jaw dislocations are usually posterior and superior dislocations
- The traditional technique: physician places 2 thumbs (padded with gauze) on lower molars with inferior and posterior force; this technique typically requires sedation, a lot of force, and risks injury to the physician.
The following 2 techniques do not require sedation and require minimal force:
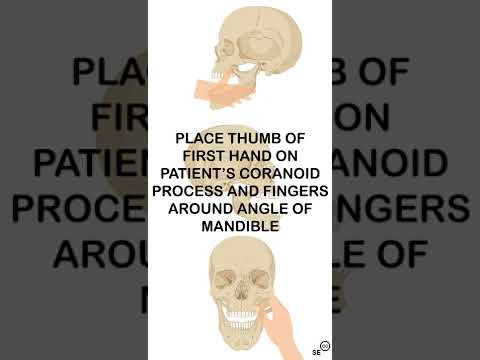
Extra-oral coronoid process TMJ dislocation reduction technique
An important anatomic landmark is the coronoid process which is not normally palpable unless dislocated.
- Have the patient in a seated position and face the patient.
- Place the tip of your thumb on the patient’s cheek and palpate the coronoid process on the dislocated side.
- Push posteriorly on the coronoid process of the dislocated side while applying an anterior force to the angle of the mandible of the non-dislocated side Place your other fingers behind the angle of the mandible for grip).
- Feel the satisfying clunk of the jaw relocating.

Syringe technique for reduction of TMJ dislocation
- Place a 5 or 10 cc syringe (based on how wide the patient can open their jaw) between the posterior molars on the dislocated side and instruct the patient rotate the syringe back and forth between their teeth until there is a clunk
- A small study of 31 patients found successful reduction in 97% of attempts using this technique with 77% reduced in < 1 minute
- An alternate technique involves placing the syringe across the molars bilaterally
- Another alternate technique involves the provider rolling the syringe back and forth while the patient bites down on the syringe

A phenotypic approach the the ED management of Crohn’s disease: inflammatory, stricturing, penetrating + anal complications
- Crohn’s disease is a chronic and progressive inflammatory bowel disease and can infect any part of the GI tract that usually manifests in the 2-4th decade of life with another peak between 50-80
- There are 3 main phenotypes of the disease: inflammatory, stricturing, and penetrating; each phenotype is associated with certain ED presentations which can help emergency physicians identify a Crohn’s related presentation, choose the appropriate work-up and management, and communicate effectively with gastroenterologist consultants
- In addition to the 3 phenotypes, anyone with Chrohn’s may have perianal disease characterized by abscesses and fistulas in the anal area or extra-intestinal features such as skin, musculoskeletal, and ocular complications
- The most common causes of Crohn’s disease exacerbations are: medication non-compliance, NSAID use, antibiotics, and smoking
Inflammatory phenotype of Crohn’s
- Typically presents with increased stooling frequency, loose bowel movements, and rectal bleeding
- The differential diagnosis includes infectious diarrhea and c difficile, especially if there is a history of recent antibiotic use
- Additional work-up includes stool C&S/O&P/C. diff toxin and fecal calprotectin if available
- Treatment may include oral prednisone 40 mg daily x2 weeks then 5 mg taper per week; consider budesonide for distal small bowel disease
- CT abdomen/pelvis is generally not indicated
Stricturing phenotype of Crohn’s
- Typically presents with signs and symptoms of bowel obstruction including increased abdominal pain, nausea/vomiting, bloating, and obstipation
- The differential diagnosis includes incarcerated hernia, volvulus, adhesions, and malignancy
- A CT abdomen/pelvis should be obtained to assess for bowel obstruction and to rule out alternate causes
- The treatment will likely involve surgical consultation +/- steroids
Penetrating phenotype of Crohn’s
- Typically presents with intraabdominal abscess(es) or fistula(s)
- The differential diagnosis includes perforated diverticulitis, appendicitis, malignancy, and post-operative complications
- Include CT abdomen/pelvis, blood cultures, and urinalysis in the work-up
- Treatment involves antibiotics and surgical consultation; avoid steroids in patients with penetrating Crohn’s exacerbation
Perianal disease in Crohn’s
- Presents as anal discharge, anal abscess(es), anal pain
- The preferred imaging is with an MRI; due to limited availability, CT pelvis and/or examination under anesthesia by a surgeon may be warranted
Bottom line => Crohn’s disease presentation, investigations, and management can be organized into 3 phenotypes + perianal disease. All patients should be assessed for potential complications, but CT scan should be limited to patients with suspected stricturing or penetrating complication or other potentially surgical pathology. Disposition will depend on the symptoms, a patient’s ability to tolerate PO intake, complications, and specialist consultation advice.
Approach to effective analgesia in renal colic and preventing bounce backs
- Ureteric stones cause pain when ureteric stretch induces release of prostaglandins leading to vasodilation and diuresis, thereby increasing intrarenal pressure, leading to painful spasms
- NSAIDs target this mechanism of pain by inhibiting prostaglandins
- Evidence from multiple studies suggest that NSAIDs are as efficacious, if not more efficacious, than opioids for pain relief in renal colic and act quickly with less side effects; however, 1/3 of patients have inadequate pain control with NSAIDs alone
- Administering NSAIDs with opioids results in more effective pain relief and decreased need for rescue analgesia
- There is no good evidence for the use of antihistamines, antispasmodics, fluids, dexamethasone, or acupuncture
- NSAIDs can be delivered IV, IM, PO, or PR
- The IV route is associate with faster analgesic onset than PO and rectal, with a slightly higher rate of adverse events
- IM ketorolac is painful and should be avoided whenever possible
- Rectal NSAIDs are a good option for patients who cannot tolerate PO and in whom IV placement is delayed or fails
- The ceiling dose for IV ketorolac is 10 mg and the ceiling dose of ibuprofen is 400mg based on ED RCTs; higher doses are associated with increased adverse side effects with no added benefit
- The initial dose of IV morphine is often under-dosed in practice, often resulting in repeated under-dosing; the recommended initial dose of IV morphine is 0.1 mg/kg (i.e. 7 mg in a 70kg adult)
- If a patient has a strong contraindication to NSAIDs, give acetaminophen instead (diabetes and mild CKD are not absolute contraindications for single dose NSAID use)
- Some other considerations when prescribing NSAIDs are:
- COX-2 inhibitor or concurrent PPI for those with GI risk factors; note that reviews have shown that COX-2 inhibitors are associated with increased cardiovascular risks in specific patient populations
- Naproxen has fewer cardiac adverse events compared to other NSAIDs
- Ibuprofen has fewer renal adverse events compared to other NSAIDs
Bottom line => Always treat renal colic with an NSAID (unless strong contraindication) +/- and opioid at appropriate doses. On discharge, provide a prescription for the most appropriate NSAID for that patient, acetaminophen, and consider a short course (no more than 5-10 tablets) of an opioid such as morphine 5mg 1-2 tabs q4h prn for breakthrough pain to prevent re-presentations for inadequate analgesia to the ED.
Inhaled steroids for asthma after ED visits – a missed opportunity
Inhaled steroids as controller therapy improve lung function and symptom control, reduce airway inflammation, the risk of exacerbation, the need for an ED visit, and total exposure to systemic steroids.
A 2021 Cochrane review (Crossingham et al., 2021) of 5 studies with 9657 patients evaluated combination therapy for asthma
- P: Outpatients aged 5+ with mild asthma
- I: Combination inhaler: budesonide 200 micrograms with formoterol 6 micrograms as needed
- C: Bronchodilator inhaler: terbutaline or formoterol as needed
- O: Combination inhaler reduced exacerbations requiring systemic steroids when compared to a beta agonist inhaler alone (OR 0.45), asthma-related hospital admission or ED visit (OR 0.35), and total adverse events and exposure to systemic steroids.
The literature suggests few patients receive a steroid inhaler from the ED at discharge.
A 2023 retrospective study from Journal of Emergency Medicine (Kligler et al., 2023) included 3948 ED visits of adult patients with asthma. An inhaled steroid was prescribed for only 6% of patients with asthma exacerbation discharged from the ED. For patients with two or more ED visits over 12 months, the rate was 6.7%. Plus, only 14% of these patients had follow up within 30 days.
Guidelines support the use of inhaled steroids after asthma exacerbation. The Global Initiative for Asthma 2022 guidelines recommend prescribing a regular ongoing inhaled steroid if the patient is not already on one. An inhaled steroid is the preferred first step in the management pathway for patients who are discharged from the ED, not a SABA alone. These guidelines recommend using combined budesonide with formoterol on an as needed basis for the first step in the regular outpatient management pathway for well-controlled asthma.
The National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group conditionally recommends that in individuals aged 12 years and older with mild persistent asthma should use either daily low-dose inhaled corticosteroid and as-needed short acting beta-agonist for quick-relief therapy or as-needed inhaled corticosteroid and short acting beta-agonist used together. They also recommend that patients aged 4 years and older with moderate to severe persistent asthma should use a combination steroid and beta-agonist in a single inhaler used as both daily controller and reliever therapy.
Bottom line => Consider prescribing an inhaled steroid with or without short term oral steroids in the patient who will be discharged from the ED with an asthma exacerbation. There are a variety of inhaled steroid options (e.g. budesonide 200-400 mcg or fluticasone 100-250 mcg daily). A short acting beta-agonist should be used for worsening symptoms but should not be used as monotherapy. Instruct the patient to swish with water and spit after using the steroid inhaler to prevent oral thrush.
Calcium in trauma patients – who needs replacement? The “lethal diamond”of trauma
- Observational data suggests that 50% of trauma patients are hypocalcemic on ED arrival
- Calcium levels drop for 2 reasons: bleeding and treatment of bleeding with packed red cells containing citrate
- Ionized calcium is the active version in the blood and is important for many physiologic processing including clotting factor binding and activation, platelet adhesion, and myocardial contractility; hypocalcemia negatively impacts the clotting cascade and myocardial contractility
- The lethal diamond of trauma has recently been proposed which adds hypocalcemia to the classic lethal triad of hypothermia, acidosis and coagulopathy
- Hypocalcemia is associated with worse outcomes, greater transfusion requirements and overall increased mortality
Dr. Petrosoniak’s suggested approach to calcium administration in bleeding trauma patients:
Do not give calcium empirically to all bleeding trauma patients; divide patients into 3 groups:
- In a patient with profound hemorrhagic shock, give calcium after administering TXA and starting the first unit of packed red cells; continue to administer calcium after every 3 units and use serial serum ionized calcium levels to guide your management.
- In a stable actively bleeding patient, give calcium after the second or third unit of packed red cells and after every 2-3 units of packed red cells thereafter
- In all other patients, use serial serum ionized calcium levels to guide calcium administration
Dose of calcium in bleeding trauma patients is calcium gluconate 1-2g IV or calcium chloride 1g through a central line
Bottom line => The studies to support calcium replacement resulting in improved clinical outcomes is lacking but until better data exists, calcium replacement of 1-2g calcium gluconate (or 1g calcium chloride through a central line) should be considered after every 2-3 units of RBCs or earlier if profound hemorrhagic shock






