
Written by Joseph Miller, DO
Spoon Feed
These are the take home points for emergency medicine from the AHA heart failure guidelines. There are some novel therapies for heart failure you need to know.
Why does this matter?
The AHA guidelines for management of heart failure (HF) were last revised in 2013, with a focused update in 2017. Given a shift in practice patterns and newer available research, a 2022 update was necessary. Understanding the current guidelines has an impact on how we manage these patients in the ED.
Many things old, some things new
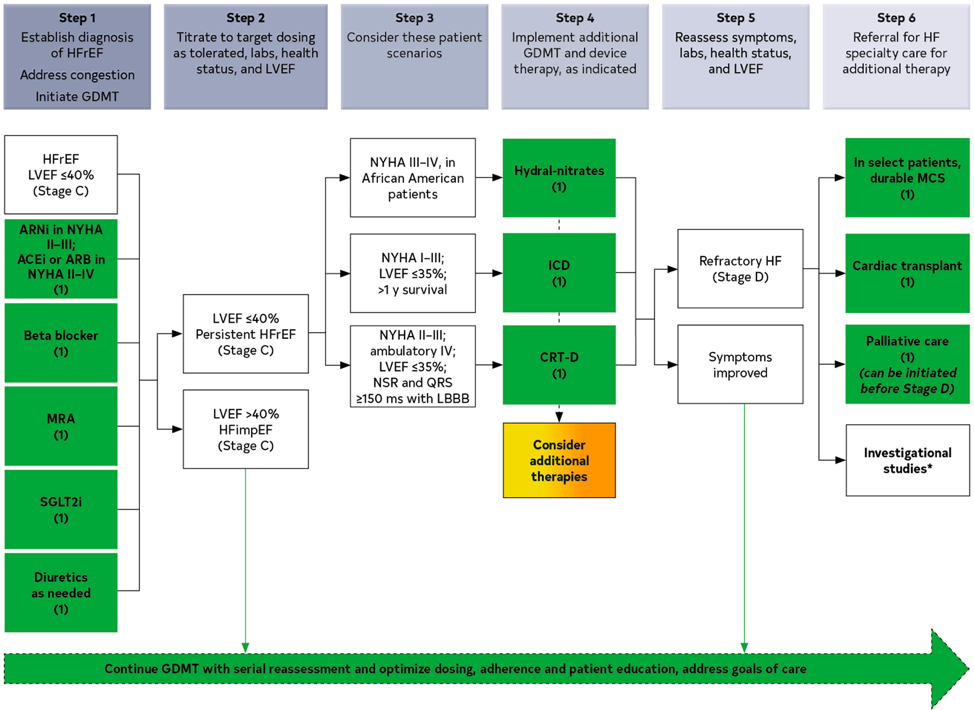
Several of the guideline revisions surround redefining HF based on recovery or persistence of ejection fraction goals. Regardless of classification, all HF patients, current and recovered, regardless of EF, should be on Guideline-Directed Medical Therapy (GDMT).
The majority of the usual HF medications are the same in the revised GDMT. A new addition is the incorporation of sodium-glucose cotransporter-2 inhibitors (SGLT2i) across several HF stages. We should familiarize ourselves with these medications and their complications, including euglycemic diabetic ketoacidosis and other diabetic complications.2
For advanced HF patients, guidelines recommend patients with terminal HF be handled by HF specialty teams for a discussion on goals of care and consideration for other treatments (heart transplant, LVAD, etc…). Their value-based assessments of these latter treatments are uncertain, but use of these management strategies has been increasing along with the complications we handle in the ED. If you need a quick primer on LVADs, see our prior post.
Other pertinent aspects of the guidelines focus on prevention of progression towards HF and management of comorbid conditions. These all certainly fall within our scope and impact our decision making when it comes to discharge planning, counseling and workup.
Here is a quick overview of the key drugs and interventions and when they are employed for HF patients.
Source
- 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 May 3;145(18):e895-e1032. doi: 10.1161/CIR.0000000000001063. Epub 2022 Apr 1. Erratum in: Circulation. 2022 May 3;145(18):e1033.
- Euglycemic Ketoacidosis as a Complication of SGLT2 Inhibitor Therapy. Clin J Am Soc Nephrol. 2021 Aug;16(8):1284-1291. doi: 10.2215/CJN.17621120. Epub 2021 Feb 9.







