
Written by Bo Stubblefield
Spoon Feed
There is a lack of evidence-based treatment standards for low-velocity gunshot wounds (GSW). This review focuses on the best available evidence for the management of civilian, low velocity GSWs to an extremity.
Why does this matter?
Remember in the 17th century when we thought infection from GSWs was secondary to gunpowder poisoning and those bullets ‘needed out’? Well, we’ve come a long way. But if you trained like I did, GSW management was/is a reality in your practice (shout out to my former co-residents in New Orleans). Here is the undeniable truth: gunshot injuries continue to increase in the United States. Yet despite the increasing frequency of civilian GSWs, the management of these injuries is debated. Specifically, while protocols for the treatment of several traumatic injuries have been developed and standardized, the optimal management of low-velocity, gunshot injuries remains uncertain.
“Shot through the arm…and it’s ok (most of the time)” – Jon Bovi
High points listed below. This article also reviews GSWs management by anatomic location (listed in Table I). Those interested should review the available evidence.
Initial Evaluation:
- Adhere to your initial ATLS surveys.
- Each would should be considered an entrance site, with number of wounds equating to number of retained bullets.
- Document a baseline neurovascular exam and obtain ankle-brachial indices (ABIs) if concern for vascular injury.
- Mark wounds with metallic markers prior to radiographic evaluation.
- Consider patient compliance when making treatment decisions, as many patients with GSWs are lost to follow up.
Antibiotics:
- Most surgeons agree that operatively treated fractures receive antibiotics.
- Debate persists regarding antibiotic regimens for non-op GSWs.
- No data exists to support superiority of oral vs. IV antibiotics.
Vascular Injury:
- Diagnose in a timely fashion and have a low threshold to obtain ABI (<0.9 gets CTA).
- ~70% of arterial injury have associated nerve injury.
- Vascular injuries may be at higher risk for infection.
Irrigation and Debridement:
- Skin healing by secondary intention is best (i.e. don’t sew up bullet holes).
- Formal wound exploration not recommended (former president William McKinley can attest).
- Removal of symptomatic subcutaneous positioned bullets is recommended.
Intra-Articular GSWs:
- Retained bullet (or fragment) should be removed to reduce mechanical wear, associated infection, and possible lead toxicity.
- In absence of retained intra-articular bullet (or fragment), evidence does not support routine articular debridement.
Table II provides grades of ortho recommendations for common management questions.
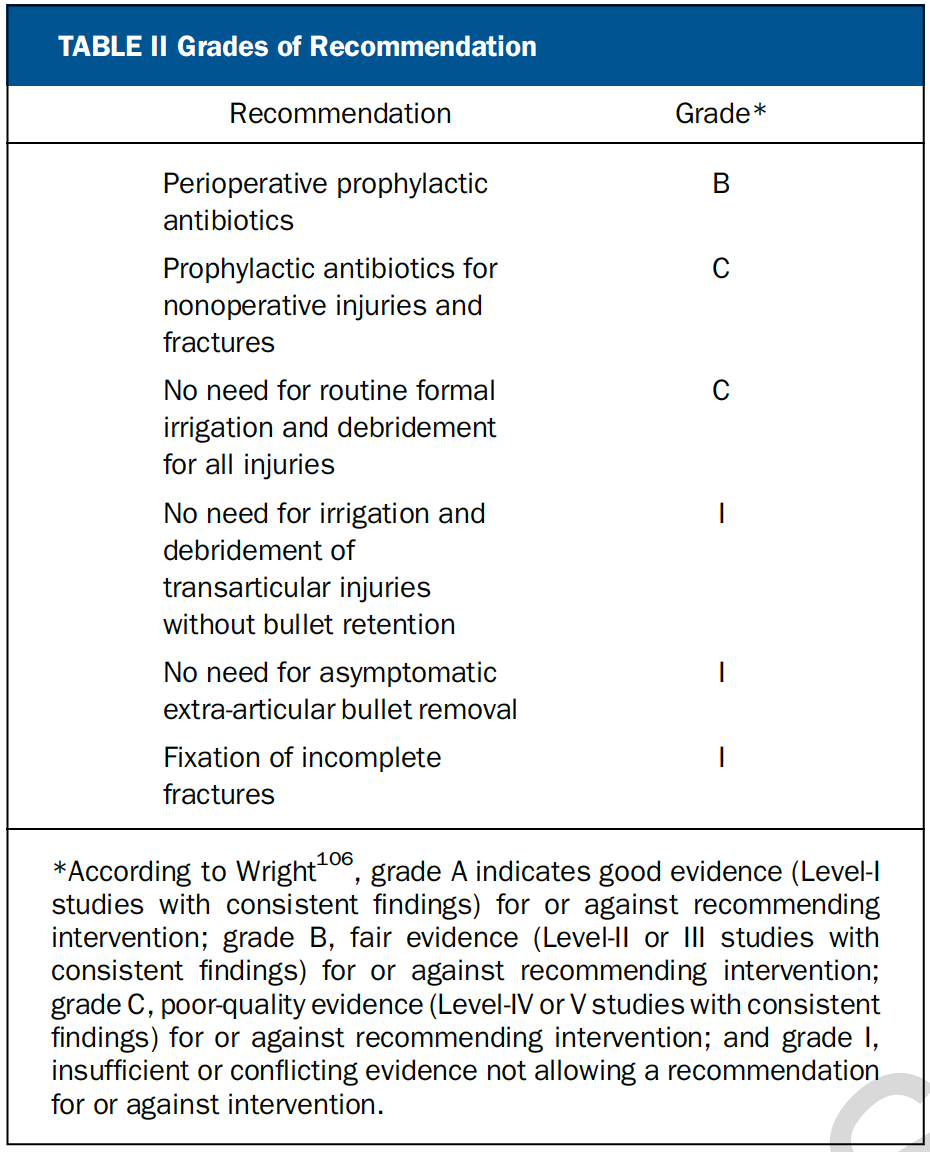
From cited article
Source
Management of Civilian Low-Velocity Gunshot Injuries to an Extremity [published online ahead of print, 2021 Mar 23]. J Bone Joint Surg Am. 2021;10.2106/JBJS.20.01544. doi:10.2106/JBJS.20.01544





