

פוסט זה זמין גם ב:
![]() עברית
עברית
Podcast: Play in new window | Download
“This learning material is sourced from Emergency Medicine Cases and has been published here with permission as per creative commons copyright”
Topics in this EM Quick Hits podcast
Justin Morgenstern on the use of high dose nitroglycerin in SCAPE (1:08)
Andrew Neill and Leah Flanagan on Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) indications and evidence (8:33)
Brit Long on indications for CT in suspected diverticulitis (26:41)
Tahara Bhate on Central Retinal Artery Occlusion (CRAO) and diagnostic error (34:47)
Matthew McArthur on penicillin allergy and penicillin challenges (42:58)
Susan Lu on how ED physician personality influences patient outcomes (52:16)
Podcast production, editing and sound design by Anton Helman
Written summary & blog post by Shaila Gunn, Brit Long, Matthew McArthur, edited by Anton Helman
Cite this podcast as: Helman, A. Morgenstern, J. Neill, A. Long, B. Bhate, T. McArthur, M. Lu, S. EM Quick Hits 56 – Nitroglycerin in SCAPE, REBOA, Diverticulitis, Diagnostic Error, Penicillin Allergy, Physician Personality. Emergency Medicine Cases. April, 2024. https://emergencymedicinecases.com/em-quick-hits-april-2024/. Accessed May 3, 2024.
High dose nitroglycerin for SCAPE – the first RCT

High-dose versus low-dose intravenous nitroglycerine for sympathetic crashing acute pulmonary edema: a randomised controlled trial by Siddiqua et al. 2024, the first RCT on this topic, suggests higher doses of nitroglycerin that are typically used are safe and effective.
- P: 52 SCAPE patients with hypoxia, hypertension, respiratory distress; all were also receiving BiPAP
- I: High dose nitroglycerin group; IV bolus nitroglycerin 600-1000 mcg followed by an infusion starting at 100 mcg/min
- C: Usual dose nitroglycerin; no bolus; nitroglycerin infusion starting at 20-40 mcg/min, max 250 mcg/minute
- O: Resolution of symptoms in 6 hours was 65% for the high dose group vs 12% in the usual dose group (NNT = 2); endotracheal intubation was 4% in the high dose group vs 19% in the usual dose group; the high dose group also had lower admission rate, shorter length of stay, fewer MACE; there was no hypotension in either group; the usual dose group reported more headaches compared to high dose group
Is this all too good to be true?
- Limitations: This was a small, single center, unblinded trial; even though these outcomes are largely objective, this does not mean they are not biased (i.e. only recording expected results); the results may also not be generalizable as the patients in this study were very sick
However, other literature would agree.
- Wilson et al. 2016: 2 mg (2000mcg) push doses were associated with decreased ICU admissions and only 2% having hypotension
- Matthew et al. 2021: high dose IV bolus of nitroglycerin 600-1000 mcg had no complications
- Houseman et al. 2023: Nitroglycerin infusions starting at >100 mcg/hr had a only a 4% rate of hypotension
Practical bottom line => Consider a nitroglycerin bolus dose 2-3 sprays SL (800-1200 mcg) OR IV bolus 500-1000 mcg if an IV is in place. Then start a nitroglycerin infusion at 100 mcg/min and titrate. Remember than BiPAP is another critical intervention for all of these patients.
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) – indications and evidence
This segment was written and recorded by Dr. Leah Flanagan and Dr. Liam Loughrey of The Case Report podcast, attendees of Podcast CAMP, with guest expert Dr. Andrew Neill.
REBOA is a temporizing endovascular technique to stop or control bleeding until definitive hemorrhage control is obtained.
- A potential indication includes refractory hemorrhagic shock in a patient who has arrested or is about to arrest despite optimal resuscitation
- It is done by placing a catheter into the aorta via the femoral artery, then the balloon is blown up occluding blood flow (and bleeding) distal to that site; it is a temporizing measure and does not replace the basics of resuscitation
Potential complications of REBOA
- Technical challenge: Procedurally it is similar to placing an femoral arterial line but bigger (4mm). However, the artery will be poorly perfused and it may be challenging to confirm if it is in the artery or vein. The user may not be familiar to the kit. It is made more challenging given the likely chaotic situation. In addition, the location must be confirmed prior to balloon inflation.
- Ischemia i.e. dead gut. The most commonly cited maximal time recommended to have REBOA active is 30 minutes, though this is context dependent.
- Severe reperfusion injury
- Hyperkalemia
- Opportunity cost: clinicians may inappropriately prioritize REBOA over basic resuscitation maneuvers
The evidence for REBOA is weak at best
- Castellini et al. 2021 reviewed at all available observational data and suggested that ROBOA is better than a resuscitative thoracotomy but not necessarily better than doing nothing
- UK-REBOA trial: REBOA was unhelpful and potentially harmful; this was a small trial with 90 patients; only 40% of the patients who got REBOA had the balloon inflated for unclear reasons; there was also a long tie delay between REBOA and definite control; this suggests that the centers performing this may not have been well set up to use REBOA optimally, likely reflecting a failure of the optimal use of REBOA rather than REBOA itself
Practical bottom line => REBOA is a possibly helpful technique in refractory hemorrhagic shock but it does not replace the basics of resuscitation. It’s optimal use requires a highly functional team who is familiar with it and a hospital system that can coordinate definitive control within an optimal time frame.
An approach to the workup of diverticulitis – who needs a CT?
Background:
- WBC elevated in 50% of patients with diverticulitis
- CRP elevation correlates with disease severity and complications
- First line imaging test is CT abdomen– >95% sensitivity and specificity
Indications for CT abdomen in acute diverticulitis guidelines
- World Society of Emergency Surgery guidelines 2020: Recommends imaging with CT for definitive diagnosis and they suggest against using history and exam alone.
- American Society of Colon and Rectal Surgeons Clinical Practice Guidelines 2020: Use history, exam and labs in the evaluation, but CT is the best means of diagnosing diverticulitis; CT also recommended for evaluating disease severity and determining the appropriate treatment.
- American Gastroenterological Association 2021 guidelines: Use CT to confirm the diagnosis of diverticulitis if there’s been no prior imaging confirmation; use CT to evaluate for potential complications in patients with severe presentations, those who fail to improve with therapy, are immunocompromised, or who have multiple recurrences and are contemplating prophylactic surgery in order to confirm the diagnosis and location(s) of disease.
- American College of Radiology ACR Appropriateness Criteria 2023 recommendations: Imaging may not be necessary in certain patients with typical symptoms of diverticulitis, a prior history of diverticulitis with similar symptoms, and no evidence of complications. There has been a trend towards imaging with CT to confirm the diagnosis of diverticulitis, evaluate the extent of disease, and detect complications before deciding on appropriate treatment.
- American College of Physicians 2022: Obtain CT if there’s diagnostic uncertainty. If the patient has LLQ pain and diverticulitis is suspected, start with history, exam, and labs. If the diagnosis is uncertain, or there if there’s any concern for complication, if they’re immunosuppressed, or their critically ill, obtain CT.
Practical bottom line => CT has a role in specific patients and is not required for every patient in whom diverticulitis is suspected. If diverticulitis is at the top of the differential, the patient is well appearing and PO tolerant, symptoms are controlled, no history of immunocompromised state, no sepsis, and they have a prior episode of diverticulitis with similar presentation => discharge using shared decision making and tight follow up is reasonable. If the diagnosis is uncertain, the patient is toxic or immunocompromised, or there’s concern for a complication => order the CT.
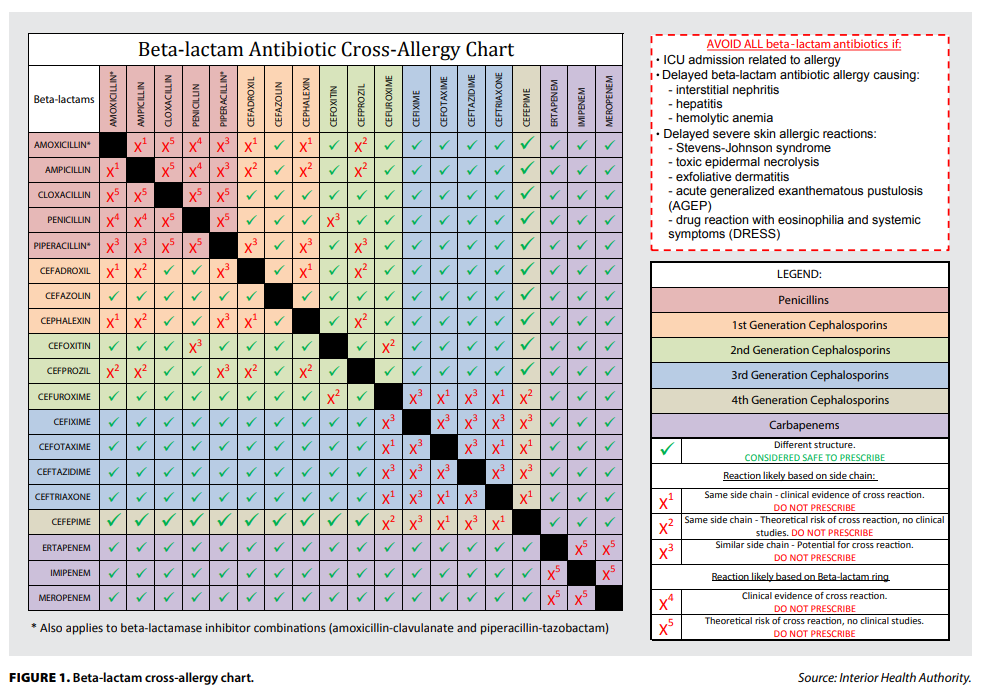
Penicillin allergy: Who can we safely provide a prescription or challenge dose to?
Allergic reactions to beta lactams are usually caused by the drug’s side chain structures, not the core beta lactam ring. Therefore, you should determine risk of cross reactivity using a cross-reactivity chart when prescribing beta lactams in a patient with known or suspected beta lactam allergy.
Prevalence and harms of erroneous penicillin allergy label
- About 90% of patients who report penicillin allergy can tolerate penicillin with no reaction
- The high rate of erroneous allergy label is due to many reasons
- Misattribution of infectious rashes to penicillin
- The strong tendency for penicillin allergy to fade with time
- Some may report allergy after side effects such as diarrhea
- Some may avoid penicillin due to a family history of penicillin allergy
- The high rate of erroneous allergy label is due to many reasons
- Penicillin allergy labels are harmful to patients
- Labeled patients receive less effective treatments and have higher rates of complications like MRSA and C. Diff, more expensive treatments, longer length of stays, and higher mortality.
Penicillin allergy de-labelling protocols
Patients at very low risk of allergy can be safely prescribed penicillin or offered a challenge dose using validated tools/calculators; very low risk: have never taken penicillin, have tolerated penicillin since the last adverse reaction.
- Point of Care Assessment Tool on dropthelabel.ca
- PEN-FAST Score for estimating risk of penicillin allergy, available on MD Calc: https://www.mdcalc.com/calc/10422/penicillin-allergy-decision-rule-pen-fast. More points = high risk
- F – less than five years since reaction
- A – anaphylaxis or angioedema
- S – severe cutaneous symptoms
- T – treatment required
Who can be safely offered an oral challenge dose or be prescribed penicillin?
- Adults receiving penicillin >10 years ago with an isolated cutaneous symptom without severe symptoms or need for resuscitation
- Children with delayed onset rashes (> 2 hours after a dose or lasting >24 hours) without serious or systemic symptoms
The risk of minor skin reaction using oral protocols is around 5%. The risk of serious reaction/anaphylaxis is extremely low and likely comparable to baseline risk.
Practical bottom line => Most penicillin allergies are erroneous and the label is potentially harmful to patients. You do not need to be an allergist to evaluate or de-label someone at low risk of penicillin allergy. De-labeling is a simple intervention which can improve patient outcomes and antimicrobial stewardship in your community.
ED physician personalities may impact patient outcomes
The most commonly used model of personality traits is the Big 5 Model, which can be remembered by the mnemonic OCEAN.
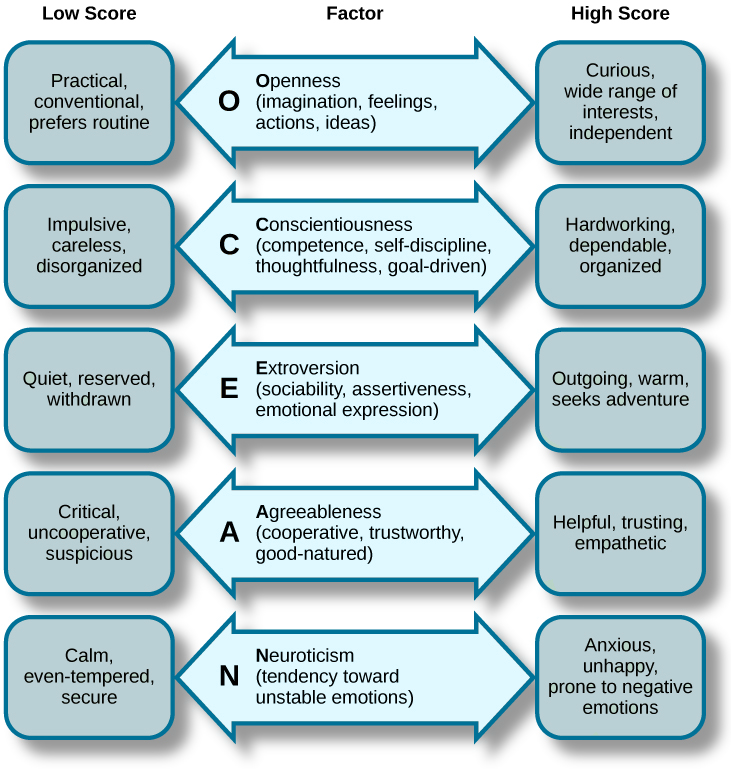
Patient outcomes (in-hospital mortality rates, medical expenditures, length of stay) were predicted by 3/5 of these traits in the ED:
- Openness: Physicians with higher openness scores have lower in hospital mortality rates, lower lab test costs, and shorter lengths of stay. They are more likely to adopt new techniques and technologies.
- Agreeableness: Physicians who are agreeable are more likely to help patients save lab test costs, especially if they are low income. They were more empathetic towards patients.
- Conscientiousness: More conscientious doctors had more lab test costs, made patients wait longer before procedures, and had longer wait times. They are careful and thorough, but there was no significant difference in patient outcomes.
Practical bottom line => ED physicians personality traits, specifically openness, agreeableness, and conscientiousness, may affect patient outcomes in the ED setting. Physicians and administrators should be aware of these traits when training physicians.

