
Written by Davin Brar
Spoon Feed
Adenosine is not just a therapy for regular narrow complex tachycardia. It can also be an important diagnostic tool to determine the etiology of the arrhythmia.
Why does this matter?
The ED is usually the first point of contact for patients presenting with arrhythmias. Timely and accurate diagnosis is important, especially as the etiology of the rhythm disturbance ultimately guides further management and disposition. Specifically, regular narrow complex tachycardia can be caused by various benign and pathologic rhythms: sinus tachycardia, atrial flutter, AV nodal reentry tachycardia (AVNRT), AV reentrant tachycardia (AVRT), etc. We commonly utilize adenosine to treat patients with SVT, but can it help clinch the diagnosis as well?
It’s all about the P…. waves
Standard treatment modalities for patients with stable SVT include vagal maneuvers, adenosine, beta blockers, or calcium channel blockers. Although the initial management of SVT is relatively straightforward, it can frequently be difficult to differentiate the exact cause of SVT. However, there are ECG findings that may help establish the diagnosis, some of which are more apparent after adenosine administration.
Two common causes of SVT include AVNRT and AVRT. AVNRT occurs from a reentry circuit around the AV node. On the other hand, AVRT is due to an anatomic accessory pathway that can lead to a reentry circuit between the AV node and the accessory pathway. AVRT can be orthodromic or antidromic. Orthodromic AVRT produces a regular narrow complex tachycardia (NCT) due to the anterograde conduction in the AV node and retrograde conduction through the accessory pathway. Antidromic AVRT produces a wide complex rhythm because anterograde conduction occurs via the accessory pathway. Unfortunately, orthodromic AVRT can often be difficult to distinguish from AVNRT.
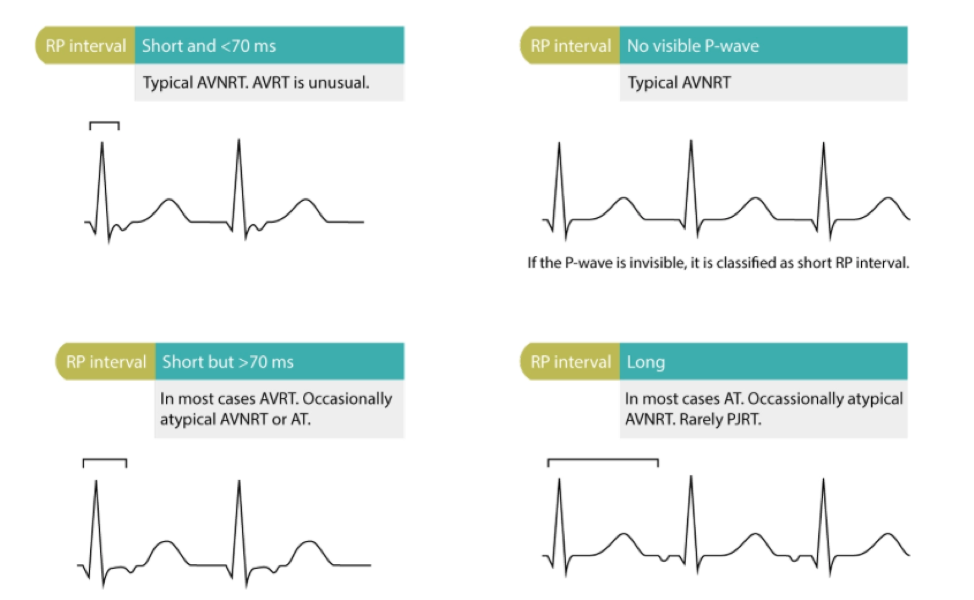
The RP interval on the EKG can be used to differentiate AVNRT from AVRT. In AVNRT, retrograde P waves occur early so they usually are not seen or are part of the QRS (appearing similar to a R’ wave at the terminal portion of the QRS). AVRT differs in that the retrograde P waves occur later (RP interval is longer >70 msec). Please see the figure below for a visual representation.
After adenosine administration, it is important to note the mode of termination on continuous ECG. Continuous EKG recording should always be used when administering adenosine to monitor for rhythm changes that can help distinguish between different types of supraventricular tachycardia (SVT). Typical AVNRT or orthodromic AVRT both terminate with a P wave indicating an AV nodal dependent tachycardia, whereas atypical AVNRT and focal atrial tachycardia terminate with a QRS complex. By inducing AV nodal block, adenosine can also help unmask preexcitation in the beats after tachycardia termination and assist with diagnosis of accessory pathways.
It is important to note the rapid half-life of adenosine (10 seconds) and proper administration. Dosages range from 6-24 mg and should be administered quickly followed by a saline flush while the rhythm is being recorded.
Edited and Peer-Reviewed by Sam Parnell
Source
Narrow Complex Tachycardias-Therapeutic and Diagnostic Role of Adenosine. JAMA Intern Med. 2022 Apr 1;182(4):436-437. doi: 10.1001/jamainternmed.2021.7764.







