
בסוף הפרסום יש בקשה למשוב
A 62-year-old male with a past medical history of osteoarthritis presents to the ED with bilateral lower extremity weakness. He states that for the last few months, he has had an increasingly difficult time climbing stairs. He notes progressively worsening neck pain and stiffness for the past year. This morning, his wife urged him to come in because she noticed he was having trouble holding a cup of coffee in his hand.
Vital Signs
HR: 83
BP: 114/68
RR: 16
O2: 98% on room air
Temp: 37C
General: Appears mildly uncomfortable. Sitting upright in a cart
HEENT: Pupils equal, round, reactive to light and accommodation, extra-ocular movements intact.
Cardiac: Regular rate and rhythm
Pulmonary: Clear to auscultation bilaterally
Abdominal: Soft, non-distended, non-tender
MSK: Midline neck tenderness at the level of C5 without step-offs, visible discomfort with range of motion of the neck
Neuro: Cranial Nerve (CN) 2-12 intact, weakness with bilateral hand grip, 5/5 strength bilateral upper extremity flexion and extension, 4/5 strength in hips bilaterally, 5/5 strength with knee and ankle flexion and extension. Sensation intact to light touch throughout. Bilateral knee hyperreflexia. Upgoing Babinski.
Labs unremarkable, including ESR and CRP.
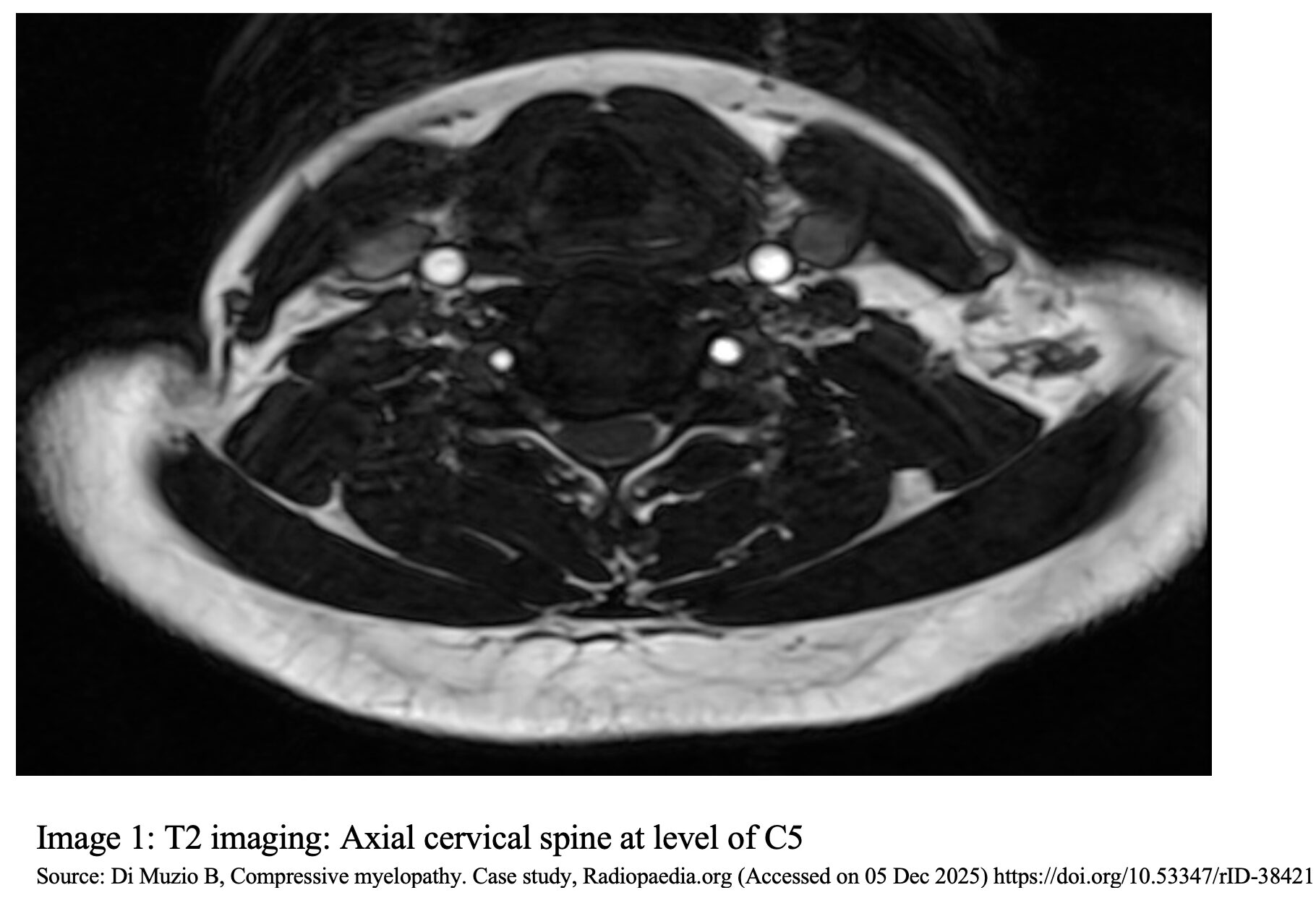
MRI Cervical spine: T2 imaging at the level of C5 with a hypo-intense signal surrounding the cord and flattening of the central cord, giving a kidney bean appearance (image 1)
Question: What is the diagnosis?





