-
Evidence Based COVID
-
Updated: 3/29/2020
Keck School of Medicine of USC
COVID-19 Evidence-Based SummaryFor questions or corrections, email: mhochman@med.usc.edu
Table of Content
Section 1: What’s new this week……………………………………………………….1
Section 2: Epidemiology, Incubation and Transmission………………………….……2
Section 3: Clinical Care……………………………………………………………………4
Presentation, diagnosis, treatment, ICU care, prognosis and outcomes
Pediatrics, pregnancy, breastfeeding, and the elderly
Palliative care and ethical considerations
Section 4: Protecting Healthcare Workers …………………………..………………….9
Personal protective equipment and hospital precautions
Airway management and intubation and managing exposures in healthcare settings
Section 5: Health System Best Practices …………………………..………………….10
The Four S’s of Disaster Relief Planning
Primary/Outpatient Care (Telemedicine)
Surgery
Supplemental Resources
Section 6: Virology, Drug and Vaccine Development…………………………………12
Virology and drug targets
Vaccine development
Section 7: Public Health Simulations………………………………………………..13
Modeling and predictions, simulations using “suppression” and “mitigation approaches”, estimating ICU needs
Acknowledgments……………………………………………………….………….14
Section 1: What’s new this week?
Point of care test approved: FDA approved an Abbott Labs point-of-care COVID-19 test, offering results within several minutes.
Discontinuation of home isolation: New CDC guidance indicates that home isolation may be discontinued 72 hours after resolution of fever and respiratory symptoms and at least 7 days have passed since symptoms appeared. Alternatively, isolation may be discontinued after symptom resolution and two negative tests 24 hours apart. A new analysis showing that the virus remains detectable for up to 8 days after symptoms raises concerns about this approach, however.
Loss of Smell: A new statement from the American Academy of Otolarygology indicates that “anecdotal evidence is rapidly accumulating … that anosmia and dysgeusia are significant symptoms associated with the COVID-19 pandemic. Anosmia .. has been seen in patients ultimately testing positive for the coronavirus with no other symptoms … these symptoms may be added to the list of screening tools for possible infection”.
Chloroquine/hydroxychloroquine suggested as treatments: Though rigorous clinical trial data are not yet available, in vitro data and now some clinical studies suggest a potential benefit for chloroquine/hydroxychloroquine in treating COVID. Other studies have not demonstrated a benefit, however, and there are safety concerns with these medications. Meanwhile a small study showed benefit when combining hydroxychloroquine with azithromycin. Despite the limited data, some clinicians are treating patients — particularly those who are in the ICU — with these medications.
Convalescent serum: FDA has approved convalescent serum for COVID-19 treatment under an emergency Investigational New Drug (IND) application. A small uncontrolled preliminary study shows encouraging results.
Personal Protective Equipment: CDC has suggested strategies to optimize supply of facemasks, including use of homemade masks; FDA issued guidance on preserving, specifically gloves and ventilators.
Resource allocation: A NEJM article provided 6 recommendations regarding allocation of scarce resources during a pandemic: 1) maximizing benefits of resources; 2) prioritizing care for front-line healthcare workers; 3) not to allocate based on a first-come, first-serve basis; 4) respond quickly to evidence; 5) recognize research participation; and 6) applying same principles to COVID and non-COVID patients.
Cardiovascular involvement: According to a new JAMA article, myocardial injury is significantly associated with fatal outcome of COVID-19, while the prognosis of patients with underlying CVD but without myocardial injury is relatively favorable. Myocardial injury is associated with cardiac dysfunction and arrhythmias.
Section 2: Epidemiology, Incubation and Transmission
Infection Burden
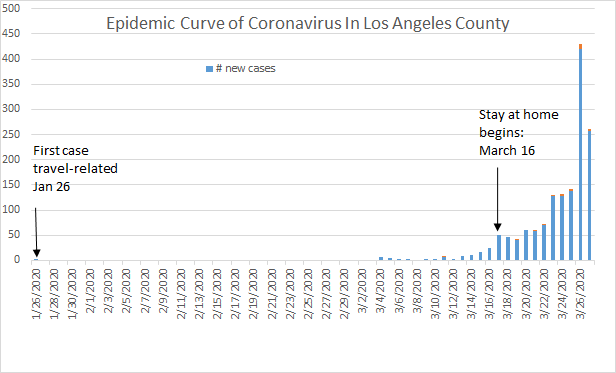
L.A. County: Current LA County Numbers and interactive city and community level map
As of 12:00PM, March 27: L.A. County has 1,465 cases and 26 deaths, with 317 hospitalizations.
Characteristics of 1,402 cases: 2% in ages 0-17 yrs, 39% in ages 18-40 yrs, 40% in ages 41-65, 19% in ages >65 yrs.
As of March 18, 2,145 people had been tested in L.A. County and 10% were positive and 28% of these had been hospitalized.
As of the week of March 23, influenza was still circulating in L.A. County as a possible differential diagnosis, although it is beginning to decline.
Case-fatality rates increase with age, at 0.2% in 10-19 yrs, 3.6% in 60-69 yrs, 8% in 70-79 yrs, and 14.8% in those 80 yrs and older, based on data from China.
Case-fatality rates are higher in persons with underlying conditions: hypertension, diabetes, cardiovascular disease, chronic respiratory disease and cancer.
Although older age is a stronger risk factor for severity and death, poor outcomes are also seen in younger patients, especially those over 50 and those with underlying conditions.
U.S.: As of March 27, 85,536 cases and 1,246 deaths; , latest data here: CDC
Worldwide: As of March 27, 590,594 cases and 26,943 deaths, latest data here: JHU Map
Incubation
Most cases occur 4-5 days after exposure, but there’s an estimated range of 2-14 days.
Median of 4 days (IQR= 2-7 days), 1099 Chinese cases through 1/29/20.
Median ~5.1-5.2 days, 97.5% will develop symptoms within 11.5 days.
Transmission
Person-to-person transmission occurs mainly via respiratory droplets, similar to influenza, and thus droplet precautions are recommended.
There may be some airborne spread of COVID, see CDC guidance on reducing risk.
COVID-19 can live on surfaces for up to 72 hours (plastics, stainless steel).
NEJM paper suggests the virus can remain viable and infectious in aerosols for hours.
Fecal-oral transmission doesn’t appear significant– this issue is not settled, however.
Studies report secondary spread rates of 1-5% and 0.45%.
Asymptomatic/presymptomatic individuals may still harbor high viral loads, and there may be some pre-symptomatic and asymptomatic spread. Though unresolved, some estimates indicate substantial transmission by asymptomatic/presymptomatic individuals.
New data from Japan reports the proportion of asymptomatic COVID-19 patients ranged from 17.9% (95%CI=15.5-20.2) and 30.8% (95% CI: 7.7-53.8).
Section 3: Clinical Care
Clinical Presentation
COVID-19 presents similarly to many other viral respiratory infections.
In a study of 138 hospitalized patients in Wuhan, initial symptoms were as follows:
Fever in 99% (In another study, however, fever was present in only 44% of patients on admission, though 89% experienced fever during the hospitalization).
Fatigue in 70%
Dry cough in 59%
Anorexia in 40%
Myalgias in 35%
Dyspnea in 31%
Sputum production in 27%
Contrary to earlier reports, digestive symptoms including diarrhoea may be a symptom in up to 50% of cases; patients presenting with GI symptoms may have worse outcomes.
Patients may also experience runny nose and sore throat as well as a loss of smell.
Diagnostic Testing
Testing for Covid-19 involves the reverse transcriptase-PCR.
Due to shortage of testing supplies, the FDA has begun permitting coronavirus testing using laboratory-developed tests without prior agency approval.
Criteria for who should be tested remains controversial:
Prioritize patients with serious, unexplained respiratory illness as well as those who are symptomatic with contacts of known cases.
Because of the incubation period, experts also highlight that “a negative result does not rule out infection, particularly for people with a known exposure [and a] positive result in an otherwise well or mildly ill patient does not require urgent medical attention but does require isolation …”
Actual sensitivities and specificities are not yet available.
Tests for presence of antibodies, to confirm previous infection, also in development.
Nasopharyngeal testing for COVID-19 may have limited sensitivity. In 1,050 samples from 205 patients with confirmed COVID-19, samples were positive in only 72% sputum specimens and 32% pharyngeal swabs while 29% had positive feces. However, this analysis was conducted in China during an earlier phase of the epidemic and testing methods may now be better.
Treatment
For the vast majority of COVID-19 cases, treatment includes supportive care.
ACEi/ARBs/NSAIDs: SARS- CoV-2 utilizes ACE2 for binding, which raises a potential role for ACEi/ARBs/NSAIDs, all of which impact ACE2.
Because NSAIDs may upregulate ACE2, some have questioned their safety in patients with COVID-19. While some organizations are calling for further evaluation, the WHO doesn’t recommend avoiding NSAIDs.
Because of their effects on ACE2, some have hypothesized that ACEi/ARBs may be harmful, while others have suggested their use as a therapeutic option. A clinical trial has been proposed to evaluate their use in treating COVID-19.
In the interim, the ACC/AHA released a statement that patients should continue on these agents for now as the situation is assessed.
Hydroxychloroquine/Chloroquine: Because of its interaction with ACE2 and potential to block viral growth, chloroquine was first studied in the SARs outbreak. Now with COVID-19, hydroxychloroquine/chloroquine are being studied again. Preliminary evidence shows their therapeutic potential. Though rigorous clinical trial data are not yet available, in vitro data and now some clinical studies suggest a potential benefit for chloroquine/hydroxychloroquine in treating COVID, while other studies have not. Despite the limited evidence, hydroxychloroquine is now being used for treating patients, though this is not an FDA-approved indication.
Hydroxychloroquine and Azithromycin: A small non-randomized study has suggested a benefit of combining hydroxychloroquine with azithromycin for treating COVID-19. Given that hydroxychloroquine/chloroquine and azithromycin are currently under investigation, they are not FDA-approved for COVID-19 and caution is advised.
HIV protease inhibitors: Lopinavir-Ritonavir (Keletra) is being investigated, but in the most recent study it failed to show improvement over standard of care. More promising may be the nucleoside analog Remdesivir, which was theorized to be effective in MERS and has been advocated for its use in COVID-19. While Remdesivir is currently in clinical trial, it may be used for “compassionate use”.
Immunomodulators: Because emerging data points to a cytokine storm as the catalyst for severe symptoms, clinicians are investigating immunosuppressants which target IL-6. Early indication shows Tocilizumab (Actemra) to be effective in severe cases and now further studies are underway. Similarly, Sarilumab (Kevzara) is under investigation.
Convalescent serum: Serum from previously infected individuals is also being investigated for treatment. FDA has approved convalescent serum for COVID-19 treatment under an emergency Investigational New Drug (IND) application.
ICU Care
A useful overview; also see COVID-19 section of Internet Book of Critical Care as well as this Cochrane review.
Common complications include Acute Respiratory Distress Syndrome (ARDS) diffuse alveolar damage, pneumocytes with viral cytopathic effect implying direct viral damage.
Cardiomyopathy and arrhythmias which can occur late, may be multifactorial in etiology.
Clinical markers include: elevated C-reactive protein and ferritin.
Early invasive ventilation/Personal Protective Equipment
ARDSnet lung protective ventilation protocol
Prone positioning, Conservative fluid resuscitation, Early vasoactive support
Resources from European ICU including papers and blogs from Italian ICUs.
JAMA paper data from 21 ICU patients in Washington State, all patients had comorbidities, all who were ventilated (15) developed ARDS.
Prognosis and Outcomes
Prognostic factors: A review article of 53,000 patients found that the strongest predictors of disease severity were age ≥50, smoking, and co-morbidities, particularly CKD, COPD, and cerebrovascular disease. Elevated LDH, CRP and D-dimer, and reduced platelet and lymphocyte counts were associated with severe disease.
Morbidity Data for U.S. Patients: According to a CDC report focusing on U.S. patients, “ 31% of cases, 45% of hospitalizations, 53% of ICU admissions, and 80% of deaths associated with COVID-19 were among adults ≥65 years with the highest percentage of severe outcomes among persons aged ≥85 years. Only one death has been reported in a 17 year old with COVID-19; otherwise there have been no deaths in those ≤19 years. Similar to other countries, this finding suggests the risk for serious disease and death from COVID-19 is higher in older age groups (though serious morbidity is not limited to this age group). Case-fatality percentages increased with increasing age with the highest percentages (6%–27%) among adults aged ≥85 years”.
Illness severity varies considerably. In China, mortality rates have been reported ranging from 0.7% (other areas in China) vs 5.8% (Wuhan).
Distribution of China’s Cases (n=72,134):
Mild (no or mild pneumonia): 81%
Severe disease (dyspnea, hypoxia, or >50 % lung involvement on imaging): 14%
Critical disease (respiratory failure, shock, or multiorgan dysfunction): 5%.
10-20% admitted to ICU
3-10% require intubation
Overall: 2.2%
Median age of deaths: 75 years (as of Jan 25, 2020)
Time from onset of symptoms to Death: 6-41 days, Median: 14 days, shorter for those greater than 70
Pediatric Populations
Among 2,143 Chinese children with likely COVID-19, few developed severe infection:
55% asymptomatic-mild (4% asymptomatic), 39% moderate (pneumonia, dry cough, fever, lung lesions), 5% severe (fever, cough, GI symptoms, shortness of
breath, decreased oxygen saturation), and 0.6% critical (respiratory failure, heart failure, multi-organ dysfunction)
Infants (<1 year) are more likely to have severe infection (10.6%).
Children were mostly infected by household and child-to-child transmission.
Fecal-oral transmission may be possible based on studies in children.
Recommendations for COVID-19 in children address differences by severity of disease.
CDC resources regarding children and COVID-19
Pregnant Women and Breastfeeding
Limited data but pregnant women (third trimester) with COVID-19 had a similar clinical course to that of non-pregnant adults.
Preterm delivery in ~50% of pregnant women (n=32) hospitalized with COVID-19.
Studies of similar coronavirus infections (MERS, SARS) found increased fetal loss for first term infection and also observed increased preterm birth for later infection.
COVID-19 not believed to be transmitted transplacentally.
Recommendations for the care of pregnant women with a flowchart of steps in care.
CDC recommendations for care of pregnant women and breastfeeding: A mother with COVID-19 may continue breastfeeding since the virus does not appear to be present in breast milk but should “wash her hands before touching the infant and wear a face mask, if possible, while feeding at the breast.”
The Elderly
Risks increase with increasing age and comorbidities.
Comorbid cardiovascular disease increases risk of death (acute coronary syndrome due to inflammation, depressed myocardial function, arrhythmias)
In >400 hospitalized patients in Wuhan, 20% had cardiac injury with elevated cardiac biomarkers (e.g., HStroponin) and this group was older (mean 74 vs 60), half died. (https://jamanetwork.com/journals/jamacardiology/fullarticle/2763524)
US:
CDC resources for and about elderly
Nursing home in Seattle/King County: 142 cases with 35 deaths (34 residents, 1 visitor) as of 3.18.20
China:
Mortality rate for persons >59 years in Wuhan was 5.1 times that of persons 30-59 years
191 hospitalized adults, in 54 decedents, mean age 69 years while in 52 discharged survivors, mean age 52. Adjusted odds of death increased by 10% per year of age (p=0.004).
Italy:
As of March 17: 7.2% case fatality rate (1,625 deaths)
Of those who died, mean age 81+ y; 2/3 had diabetes, cardiovascular disease, cancer, or smokers.
Men more likely to die than women and younger at death
Palliative Care and Ethical Considerations
During pandemics, a triage plan should include palliative care.
WHO and CDC developed ethical guidance for pandemic influenza.
A discussion paper from the National Academy of Medicine aims to assist in healthcare planning and application of Crisis Standards of Care for COVID-19.
The Hastings Center suggests an ethical framework for healthcare institutions during the novel coronavirus pandemic by managing uncertainty with planning, safeguarding communities, and guiding practice.
Italy’s SIAARTI’s Ethics Section developed recommendations for intensive care treatments in battling novel coronavirus pandemic to aid in provider moral distress, transparency, and a consistent allocation of scarce resources.
In Italy, ethical concerns have arisen regarding patients dying alone in hospitals without family or palliative care. In the unusual case of limited ventilator resources, an article in the NEJM calls for a volunteer committee of respected clinicians and leaders to assist in decision-making regarding withdrawing ventilator support, communicating with families, and empowering an expert palliative care team to intervene in order to buffer clinicians from disabling distress, providing symptom management and family support.
A NEJM article provided 6 recommendations regarding allocation of resources during pandemic to include maximizing benefits of resources; prioritizing care for front-line healthcare workers; not to allocate based on a first-come, first-serve basis; respond quickly to evidence; recognize research participation; and applying same principles to COVID and non-COVID patients.
Section 4: Protecting Healthcare Workers
Personal Protective Equipment
Updated infection prevention advice from CDC specific for COVID
General infection precaution advice from the CDC for healthcare providers. Personal protective equipment recommendations for close patient interaction include:
N95 respirator mask if available, medical facemask if not.
N95 strongly preferred when performing aerosol-generating procedures.
Eye protection: goggles or disposable face shield that covers front/sides of face.
Gloves
Gown use is preferable but if there is a shortage they should be prioritized for aerosol-generating procedures, care activities where splashes and sprays are anticipated, high-contact patient care activities.
Before/After Work HCW Decontamination Protocol
CDC infographic on donning and doffing PPEs.
HCW need to be prioritized for testing and care else healthcare systems risk absenteeism
Hospital Precautions
Limit visitors and traffic.
Patients with known or suspected COVID-19 should be placed in a single room with a door closed and a dedicated bathroom.
Airborne infection isolation rooms should be reserved for patients who will be undergoing aerosol-generating procedures.
Caution when considering high-flow nasal oxygen or noninvasive ventilation as increased risk of dispersion of aerosolized virus.
Facilities could consider designating entire units within the facility, with dedicated HCP, to care for known or suspected COVID-19 patients.
Airway Management and Intubation
Practical guidance for precautions and preventive measures to be taken in very high-risk exposure situations such as patient intubation are linked below:
American Society of Anesthesiologists
UK Intensive Care Society, Association of Anaesthetists and Royal College of Anaesthetists
Papers in a special edition of Anesthesiology
Very practical blog with images from an ED intensivist
Message from Italian centers: practice, practice, practice before you need to do it in real life: YouTube Link
Managing Exposures in Healthcare Settings
Guidance on what to do if potential exposure occurs to a healthcare professional:
Covers potential risk of different types of exposures, what action should be taken, and what monitoring of the health care provider should occur.
Section 5: Health System Best Practices
Central challenge: Optimize use of resources for complex decision making in real time with large amounts of uncertain and incomplete data
A Checklist from HHS was developed for hospital systems planning pandemic response.
The Four S’s of Disaster Relief Planning:
Staff
Interim CDC guideline for healthcare facilities emphasizes preparation for potential personal protective equipment supply and staff shortages.
Surge planning includes anticipating absenteeism in response to contagion and planning for staff shortages, while supporting staff to prevent this
Create registries of volunteers, plans for emergency or rapid credentialing.
Coordination with military medical corp is an option to expand staffing
Clinician and staff psychosocial needs/distress must be addressed
Recognize the increased need for emotional and psychological support in staff and patients.
Consider alternate housing and childcare for workers with families at risk
Malpractice/liability for good samaritans as enacted in the State of New York
Stuff
3 C’s, conventional, contingency, crisis with protocols for blood, IV medications (antibiotics, antipyretics, o2, NS/crystalloids)
Systems to track depleted resources and share between hospitals may be helpful
Space/Structure
Increasing hospital capacity is the most commonly cited factor.
To increase “surge capacity” using “alternate sites” in the hospital, resurrect decommissioned buildings, or create temporary, mobile, modular hospitals.
Regional coalition with local, county, state health systems to coordinate bed capacity
Environmental management is also key (hand sanitizers freely available throughout the facilities, along with trash receptacles, tissues, etc).
EMTALA changes: CMS has relaxed EMTALA requirements regarding medical screening exams allowing redirection to alternative screening locations
Will need to build capacity for mortuary services as patient volume increases
Systems
Protocol: Identify, Isolate, Inform (PUI/COVID+ patients) based on CDC’s Ebola plan
Research has consistently demonstrated systems inefficiencies – namely not matching resources with needs – is a key limiting factor in the healthcare facilities’ responsiveness.
C’s: command, control, communications, coordination, continuity of operations, and community infrastructure. This is similar to the U.S. National Incident Management System
Determine capacity (what exists in present condition) and capability (increase in capacity under appropriate mobilization of resources).
Systems organization – Organizations that have dispersed, decentralized decision making tend to be more agile because they have protocols for rapid sharing of information internally and time sensitive decision making(Organization 2).
Communication: Regular updates to patients and staff needed through multiple channels (web, email, text, social media). Designated internal and external spokespeople should serve as points of contact during changing situations.
Primary/Outpatient Care:
Alternatives to face-to-face visits: Many leading professional societies and other groups have called for a shift towards telemedicine. Medicare has broadened telehealth reimbursement opportunities in response to the pandemic and waived HIPAA penalties. California requires reimbursement for telephone visits.
Many systems have telemedicine screening as the first contact for PUI/Covid-19
Apple, in conjunction with the CDC, has created a COVID-19 screening app
Knowledge sharing networks. Penn State has launched Project Echo to share expertise, best practices between specialists and smaller healthcare facilities
Practices can consider proactively identifying patients with long term health conditions and elderly to avoid interruptions in care.
Delayed care may cause a “second wave of illness” due to COVID-19.
Professional societies have suggested limiting elective medical care
Scheduling redesign: The AAP has suggested separating well vs. sick patients to separate times and spaces (ie., well visits in AM, sick visits after).
Surgery
The American College of Surgeons has called for surgeons to cancel elective cases, with guidelines for triage of various procedures. CMS has called for delaying all elective surgeries, non-essential medical, surgical, and dental procedures.
Specific guidance from other specialty societies below:
American College of Obstetricians and Gynecologists
American Society for Reproductive Medicine
Children’s Hospital Association
Supplemental Resources:
WHO: Phases of influenza pandemics
WHO: Pandemic influenza risk management
BMJ: COVID-19 Remote Assessment in Primary Care
JHU Center for Security: Top Priorities for Pandemic Preparation
CDC: Hospital Preparedness Checklist for COVID-19
Section 6: Virology, Drug and Vaccine Development
Virology and Drug Targets
Covid-19 is caused by the SARS-CoV-2 virus.
7 coronaviruses infect humans: 4 cause colds, plus SARS, MERS and COVID-19. Many also in animals, and closest relatives so far found to SARS-CoV-2 are in bats.
Spike protein on the outside of the virus binds to ACE2 and helps determine tropism (upper respiratory tract). Entry also requires a low pH step (endosome) which chloroquine blocks, hence suggested drug.
Other antiviral drugs are being evaluated for cross-reactivity against coronavirus proteins.
SARS-CoV-2 is an RNA virus, so RNA replication is also a drug target (remdesivir).
Study has identified human cell partners of 26 of the 29 unique coronavirus proteins, and lists 69 potential drugs that could target those interactions.
RNA viruses mutate rapidly–early reports of strains evolving to have greater virulence have been disputed.
Vaccine Development
The Coalition for Epidemic Preparedness Innovations (CEPI) is funding 8 vaccine trials: Curevac, Inc., Inovio Pharmaceuticals, Inc., Moderna, Inc., Novavax, Inc., The University of Hong Kong, The University of Oxford, The University of Queensland and Institut Pasteur.
First vaccine trial is Moderna’s mRNA vaccine (mRNA-1273). mRNA is injected and makes the spike protein inside the body. Using mRNA is much faster to develop than traditional recombinant or viral vector vaccines. Trial in Seattle started 16 March 2020.
Vaccine challenges:
Efficacy – will it make the right type of immunity, with an effective combination of either neutralizing antibodies or T cell responses?
Safety – some vaccines can make infections worse through eg antibody-dependent enhancement of entry into cells.
Section 7: Public Health Simulations
Without interventions, mortality in the U.S. would peak in mid-June with ~55,000 deaths per day and culminate with 2.2. million fatalities.
A model developed at USC accounting for underlying conditions and age projects 5,500 hospitalizations in the Service Planning Area covering Metropolitan Los Angeles, our main catchment area, by 100 days with a reproductive number of 2.2 and by 250 days with a reproductive number of 1.5.
Two scenarios reflecting various combinations of interventions:
Mitigation strategy: Goal is to reduce the health impact and not to interrupt transmission completely. Strategy includes closure of schools and universities, case isolation and household quarantine, social distancing of those aged over 70. Duration: 3 months.
Contact tracing: Testing, contact tracing and isolation of contacts strategies have the best chance of breaking the chain of transmission, as was accomplished in China and is being accomplished in South Korea.
Suppression strategy: Goal is to reduce the average number of secondary cases each case generates. Strategy includes closure of schools and universities, case isolation, population-wide social distancing, and household quarantine. Duration: 5 months.
With close monitoring of disease trends, possibly relax measures temporarily as things progress but will need to be maintained until a vaccine becomes available (18 months).
A suppression strategy could reduce deaths by about 49% and peak ICU beds needed by about 67%.
The U.S. needs approximately 295,000 ICU beds under the worst case scenario.
Currently, there are 96,596 critical care beds where two-thirds are likely occupied by other non COVID-19 patients.
Tsai et al. estimated assuming a 40% population infection rate, if transmission occurs over six months, need for hospital beds will be at 274% of capacity, and ICU need will be 508% of capacity.
Another simulation model from the Institute of Health Metrics and Evaluation projects that with current social distancing policies in place, peak resource need will occur in the second week of April.
At peak, demand for ICU beds is expected to exceed capacity by about 25%, and the US will need about 19,000 ventilators.
In California, the peak is expected to occur slightly later – in the third week of April, with an ICU bed shortage of about 300 beds (about 15% over capacity), and a need for about 1,200 ventilators.
Total number of deaths in the United States attributable to COVID-19 is expected to be 81,000.
Acknowledgements
Editors: Michael Hochman, MD, MPH; and Jeniffer Kim, PhD, MPH
Section writers (no particular order): Kashif Khan, MD; Wendy Cozen, DO, MPH; Brett Lindgren, MD; Laurene Mascola, MD; Carolyn Kaloostian, MD, MPH; Paula Cannon, PhD; Carol Peden, MD, MPH; Barbara Turner, MD, MPH; Rishi Mehta, MD; Cameron Kaplan, PhD, Rusha Modi, MD, MPH; Todd Schneberk, MD, MS, MA; and Laura Taylor, MD
Section Editors (no particular order): Albert Farias, PhD; Aneesa Motala, MPH; Michael Cousineau, DPH; and Susanne Hempel, PhD