

פוסט זה זמין גם ב:
![]() עברית
עברית
Written by Clay Smith
Spoon Feed
The distance from nostril-to-tragus minus 10mm was the best way to estimate nasopharyngeal airway (NPA) depth.
Why does this matter?
When placing a nasal trumpet (aka nasopharyngeal airway, NPA) in children, we often estimate length by picking the one that reaches from nostril-to-tragus (NT); 2015 European Resuscitation Guidelines recommend nostril-to-ipsilateral angle of the mandible (NM). An MRI anatomy study found nostril-to-tragus minus 10mm (NT-10) would theoretically be best. What is the right way to estimate so the tip is distal to the soft palate but proximal to the epiglottis (see below, between P and E)?
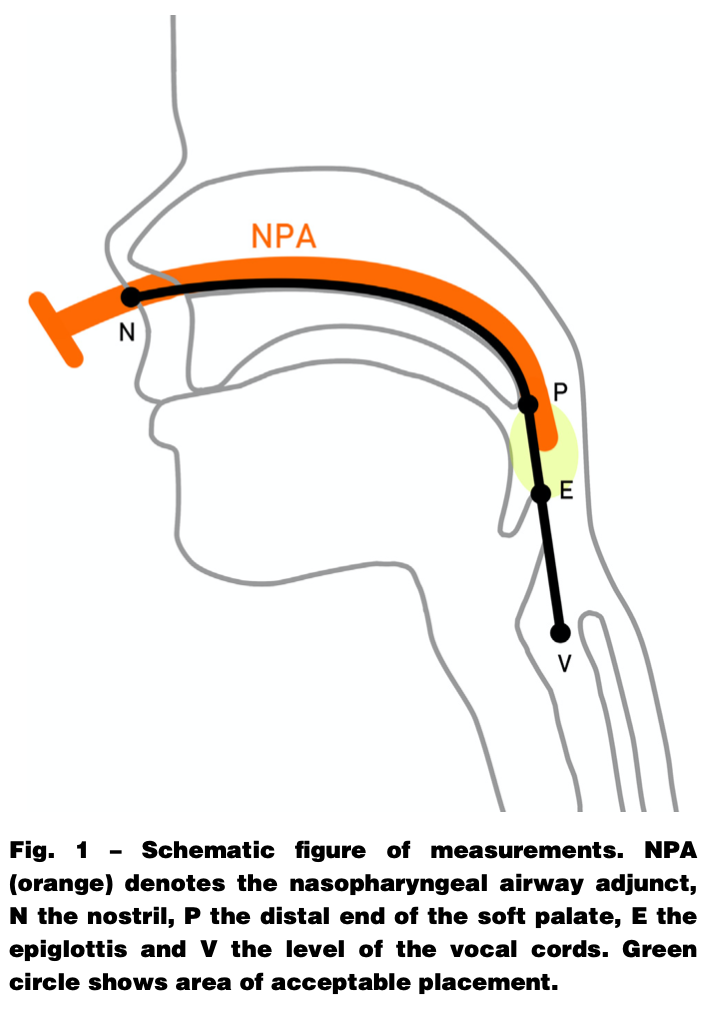
From cited article
NPA in the sweet spot
This was a prospective study of 92 children, mean age of 4 years, who were undergoing sedated MRI and had a NPA placed. The NT-10 depth resulted in the tip being between palate and epiglottis on MRI 77% of the time; 37% of the time the tip was optimally placed, very near the midpoint between P and E. There were no adverse outcomes, such as epistaxis, vomiting, or laryngospasm. They also measured NT distance while the children were sedated and found, when based on measurements on MRI, this depth of insertion would have theoretically resulted in acceptable placement in just 28.3%. For NM distance, that depth would theoretically have placed the tip acceptably in 58.7%. Based on measurements (vs actual position on MRI), the NT-10 distance would have theoretically resulted in acceptable placement in 67.4%. Of course, when actually viewed on MRI, acceptable placement was a little higher, as above, at 77%. Here is the take home point: for pediatric NPA, NT-10 is best, and even that winds up short or long up to one quarter of the time.
Source
Working with estimation-formulas to predict nasopharyngeal airway insertion depth in children: Looking at magnetic resonance images – A prospective observational study (WEND:LI-Study). Resuscitation. 2021 Sep 30;168:95-102. doi: 10.1016/j.resuscitation.2021.09.024. Online ahead of print.
