

פוסט זה זמין גם ב:
![]() עברית
עברית
Written by Ketan Patel
Spoon Feed
Presented is a process to interpret an ECG with negative P waves and pathologic Q waves in leads I and aVL.
Why does this matter?
Misinterpretations of an ECG could lead to unnecessary testing and lead down the wrong diagnostic path.
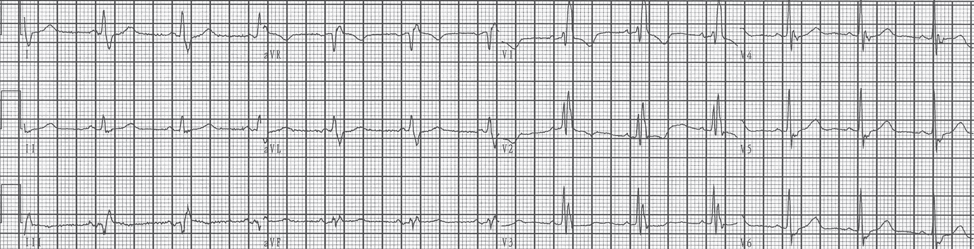
A bizarre wide complex rhythm
This article highlights a case of a 80-year-old patient who received a cardiac referral based on an abnormal ECG during a routine health evaluation.

Analysis of this ECG reveals that there is a right bundle branch block (RBBB) pattern with negative P waves (arrows) and Q waves (*) in leads I and aVL. The differential diagnosis for the vector reversal of a P wave in Lead I includes left and right-arm lead reversal, mirror-image dextrocardia, and left atrial rhythm.
Limb lead reversal results in flipping of both the P waves and QRS complexes in lead I. Leads II and III and aVL and aVR also switch places respectively, which is not the case here. Although inversion of P waves in Leads I and aVL with Q waves and negative T waves could represent a left atrial rhythm with prior lateral myocardial infarction, the patient’s history is not consistent with such.
Further analysis shows atypical conduction and reversal of right to left forces, exemplified by the reversal of amplitudes of the QRS complexes in the precordial leads. This final clue clinches the diagnosis of mirror-image dextrocardia.
When this is recognized and an ECG is performed with electrodes relocated to the respective mirror-image positions, the ECG can then be correctly interpreted as a normal sinus rhythm with a complete RBBB.
The most common type of cardiac malposition is mirror-image dextrocardia. In these patients, the right-left heart orientation is reversed, while anterior-posterior orientations are maintained. ECG clues include:
- Right-axis deviation of the P wave – Flipped P waves in aVL and Lead I, and positive in aVR.
- QRS complex activation reversal and diminishing voltage from V1 to V6.
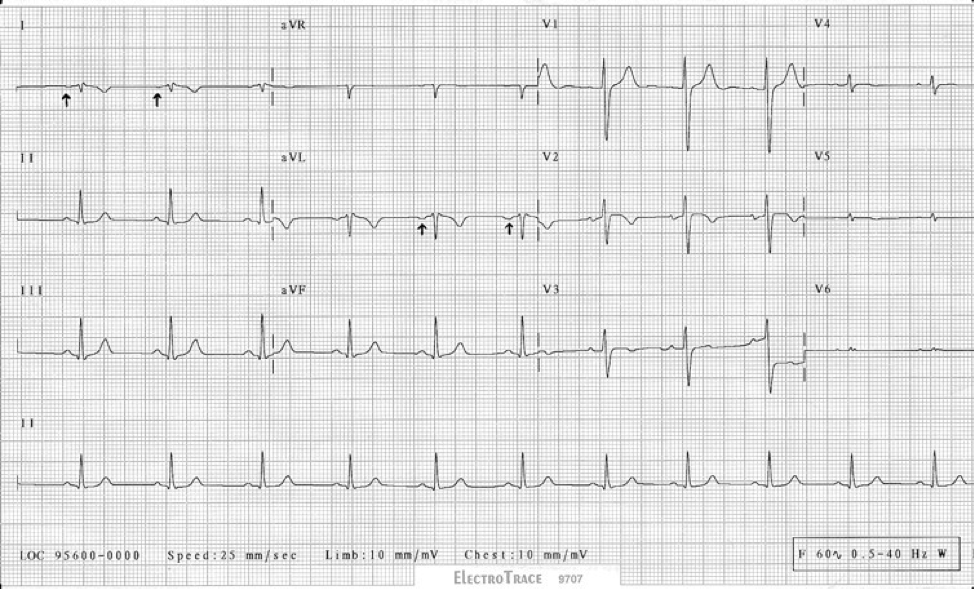
ECG C clearly highlights these clues, but as is the case of the patient presented, an arrhythmia can mask some of these findings, resulting in possible missed recognition of mirror-image dextrocardia.
Sources
- An Unusual Wide Complex Rhythm-What Is the Diagnosis? JAMA Intern Med. 2022 Jan 1;182(1):72-73. doi: 10.1001/jamainternmed.2021.6778.
- Mirror-image dextrocardia with situs inversus and coarctation of the aorta. Chest. 1974 Sep;66(3):297-9. doi: 10.1378/chest.66.3.297.
