
Podcast: Play in new window | Download
“This learning material is sourced from Emergency Medicine Cases and has been published here with permission as per Creative Commons copyright.”
Pediatric agitation in the Emergency Department is one of those presentations that can escalate quickly and leave even experienced clinicians feeling on edge. It is high-risk, resource-intensive, and often unfolds in an already overstimulating environment where small missteps can make things worse. At the same time, agitation is not a diagnosis, it is a clinical presentation that may reflect anything from psychiatric illness to delirium, intoxication, trauma, or simply a child overwhelmed by the ED itself. So how do we approach these patients in a way that is safe, systematic, and effective?
In this episode with guest experts, Dr. Susan Duffy and Dr. Thomas Chun, we tackle the questions that come up at the bedside: How do we rapidly distinguish mild, moderate, and severe agitation in a way that actually changes what we do next? Which patients are most likely to escalate, and how can we intervene early to prevent that? When should we be worried about a medical or toxicologic cause rather than assuming this is “behavioural”? What does effective verbal de-escalation actually look like in a busy ED, and why does it so often fail? When is a “code white” for emergency security measures truly indicated, and how do we avoid turning it into an escalation trigger? How should we be thinking about medications: what to choose, when to give them, and how to avoid over-sedation? And once the patient is finally calm, how do we make sure we aren’t missing the underlying diagnosis? and many more…
Podcast production, sound design & editing by Anton Helman; Voice editing by Braedon Paul
Written Summary and blog post by Sara Brade, edited by Anton Helman April 2026
Cite this podcast as: Helman, A. Duffy, S. Chun, T. Ep 217 Pediatric Agitation: Assessment and Management. Emergency Medicine Cases. April 2026. https://emergencymedicinecases.com/pediatric-agitation-assessment-and-management. Accessed May 24, 2026
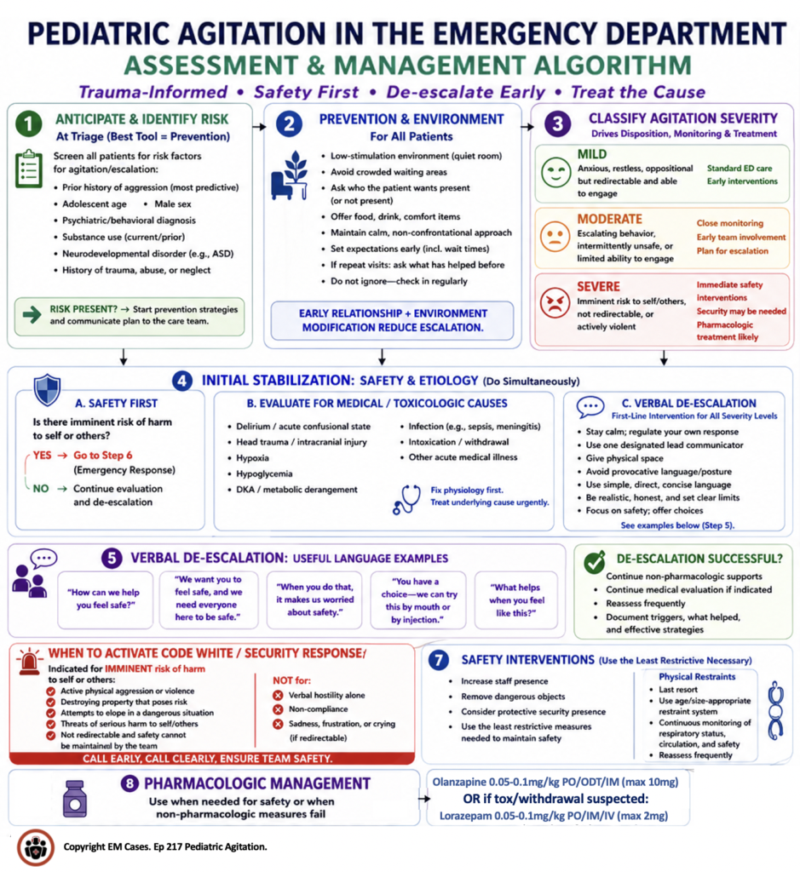
Classifying pediatric agitation in the ED as mild, moderate, or severe
The first task is to determine whether the agitation is mild, moderate, or severe, because this classification drives almost everything that follows: where the patient is placed, who needs to be involved, how closely the patient must be observed, whether urgent intervention is required, and what pharmacologic options are appropriate. Our experts emphasize that this categorization is not merely descriptive: it’s operational. It creates a shared mental model for the team so everyone can share the same level of concern and the same urgency of response.
In practical terms:
- Mild agitation: patient is anxious, restless, or oppositional but remains redirectable and able to engage with staff. These patients are appropriate for standard ED spaces with early environmental modification.
- Moderate agitation: patient demonstrates escalating behavior, is intermittently unsafe, or has limited ability to engage. These patients require closer observation, early team involvement, and proactive planning for escalation.
- Severe agitation: patient poses an imminent risk to self or others, is not redirectable, or is actively violent. These patients require immediate safety interventions, including possible security involvement and pharmacologic management.
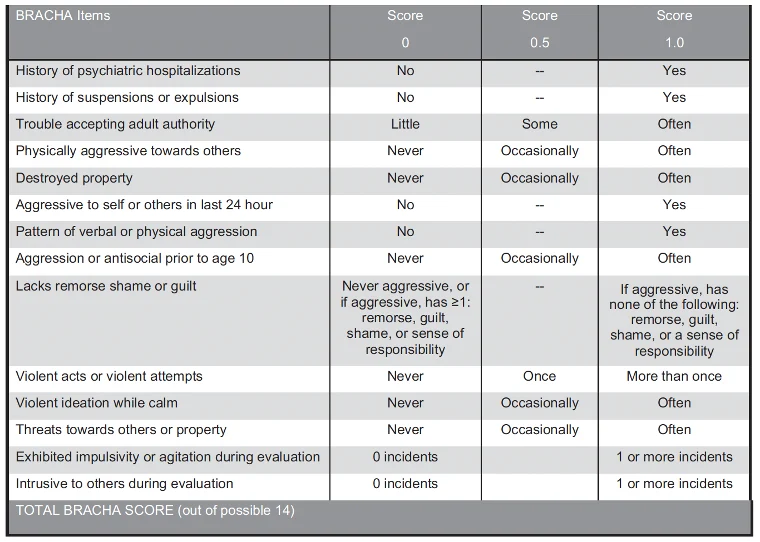
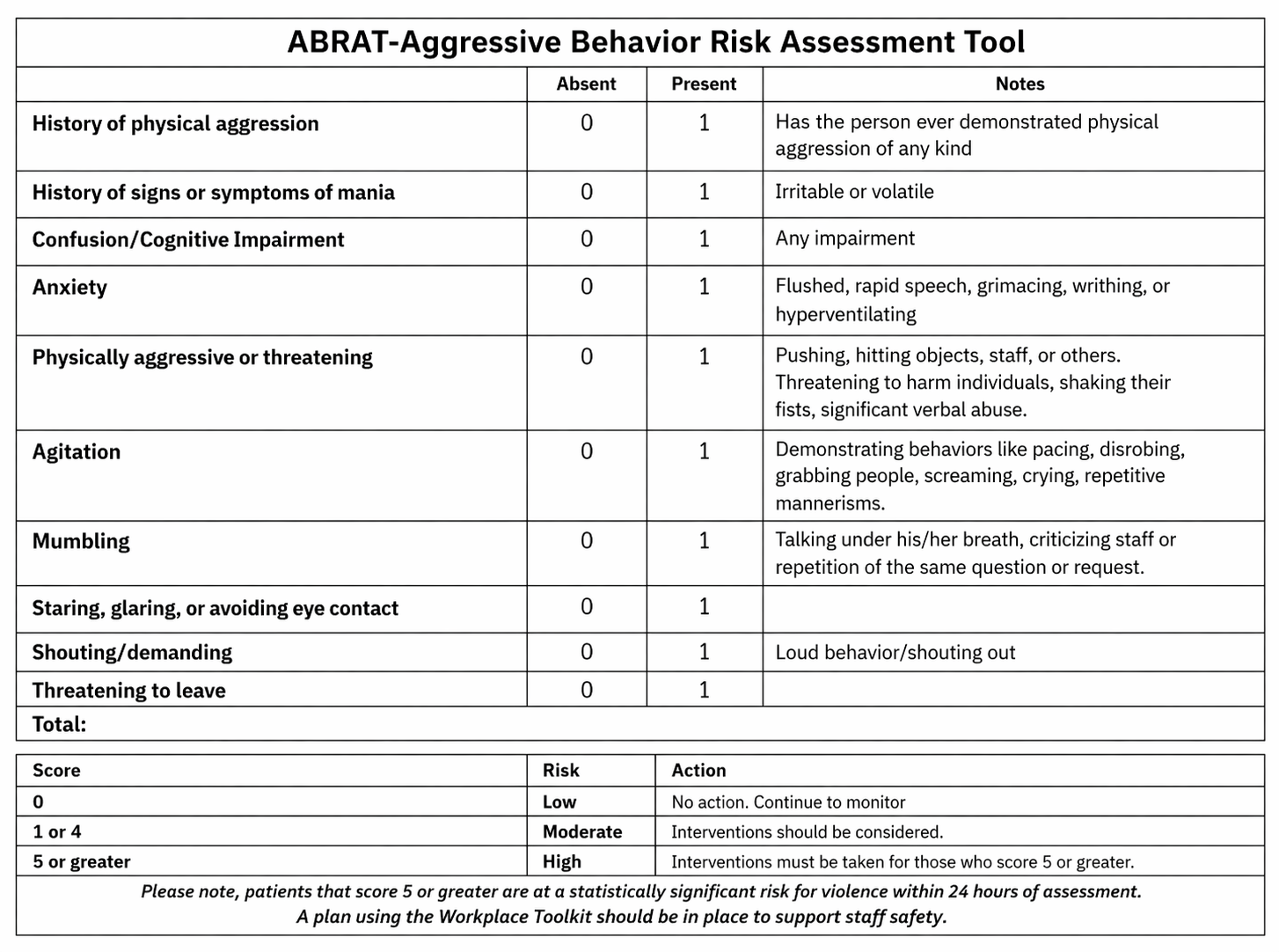
There are clinical tools such as the Aggressive Behaviour Assessment Risk Tool (ABRAT) and the Brief Rating of Aggression by Children and Adolescents (BRACHA) to guide assessment; however, our experts emphasize that clinical judgement is paramount in these cases.
Anticipating agitation: Early identification of pediatric patients at high risk of agitation in the ED
Our best tool for managing pediatric agitation in the ED is prevention. This starts at triage. Even when a child appears calm on first encounter, the team should identify red flags that suggest a higher likelihood of escalation during the ED visit.
The most predictive factor is a prior history of aggression. This is particularly important when the child has presented because of aggression at home, school, or in the community, even if they appear settled on arrival. Other important risk factors include:
- Adolescence
- Male sex
- Known psychiatric or behavioural diagnoses
- Current or prior substance use
- Neurodevelopmental disorders such as autism spectrum disorder or developmental delay
- History of trauma, abuse, or neglect
These factors influence how patients perceive the ED environment as they may be sensitive to noise, authority figures, unpredictability, and loss of control. Identification of these risk factors should trigger preventative communication and environmental modification strategies.
Using a trauma-informed approach to prevent pediatric agitation in the ED
Children with agitation often have prior experiences that affect how they respond to the ED. A trauma-informed approach means recognizing that what may look like “bad behaviour” can actually represent fear, loss of control, sensory overload, or a learned protective response.
Key early prevention interventions include:
- Place patient in a low-stimulation environment (quiet room, minimal traffic)
- Avoid crowded waiting areas
- Ask who the patient wants present (or not present)
- Offer food, drink, and comfort items
- Maintain a calm, non-confrontational approach
- Set expectations early (including wait times)
- If repeat visits, ask about and offer interventions that have been previously helpful
Pearl: Do not ignore these patients. Lack of engagement and long waits increase agitation. Regular team check-ins reduce escalation risk.
Initial stabilization of the agitated pediatric patient: simultaneous safety assessment and evaluation for medical causes
Once agitation is present, the clinician’s job is not simply to calm the child down. The more important task is to determine whether this is primarily a psychiatric or behavioral presentation, or whether there is an underlying medical cause that requires urgent treatment.
Red flags that suggest a medical or toxicological cause of agitation include:
- Delirium or acute confusional state
- Head trauma or other injury
- Hypoxia
- Hypoglycemia
- DKA or metabolic derangement
- Infection
- Intoxication or withdrawal
- Other acute medical illness
Some EDs choose critical care or high-observation areas for severely agitated pediatric patients because they are often undifferentiated and may require urgent medical assessment and monitoring.
Verbal de-escalation is the central intervention in pediatric agitation
Verbal de-escalation is a structured and team-based intervention that begins the moment the patient enters the ED and should continue throughout the entire encounter.
The foundational elements of de-escalation include:
- Stay calm and regulate your own emotional response
- Use one designated lead communicator
- Give the patient physical space
- Avoid provocative language or confrontational postures
- Use simple, direct, concise language
- Be realistic and honest about limits
- Focus the conversation on safety
- Offer choices whenever possible
Useful de-escalation language includes:
- “How can we help you feel safe?”
- “We want you to feel safe, and we need everyone here to be safe.”
- “When you do that, it makes us worried about safety.”
- “You have a choice — we can try this by mouth or by injection.”
- “What helps when you feel like this?”
When to activate a “code white” for the agitated pediatric patient in the ED
Calling a “code white” or emergency security response is one of the most consequential decisions in agitation management. This response should be reserved for cases with concern for imminent harm to self or others. It is not a response to mere non-compliance, verbal hostility, or frustration if the patient is still redirectable and not yet physically threatening.
Indications for calling a “code white”/emergency security response include:
- Imminent physical threat to staff
- Imminent risk of self-harm
- Severe agitation that is no longer responsive to de-escalation
- Need for multiple trained personnel to maintain safety
If staff are becoming increasingly concerned for safety, it is better to communicate calmly and transparently: “We’re worried about safety. We want to avoid restraints. How can we work together to keep everyone safe?” That keeps the focus on collaboration and preserves the possibility of de-escalation even as staff prepare for escalation.
Pitfall: Calling a “code white”/emergency security response is a safety response, not a disciplinary tactic. The most important pitfall is using a code white as a threat. “If you don’t cooperate, we’ll call security and hold you down” is counterproductive and often escalates the situation further. A code white should never be framed as punishment or coercion.
Use of restraints in pediatric agitation is a last resort
If physical restraint becomes necessary, it should be used only as a last resort, for the shortest possible duration, and almost always as a bridge to calming medication.
Important safety principles of physical restraints:
- Constant observation is essential
- Restraint use should follow institutional policy and time limits
- Restraints usually go hand in hand with medication
- Staff should be trained in safe restraint technique
- Prolonged restraint should be avoided whenever possible
Some pediatric centers also use structured papoose-style restraints for selected neurodevelopmental patients, or specially designed chair restraints in behavioural settings.
Pitfall: A common pitfall is prolonged and/or inappropriate use of physical restraints. Restraints are not treatment. They are a temporary safety measure while definitive calming measures take effect. The overarching principle is to use the least harmful method that safely contains the patient, and discontinue it as soon as possible.
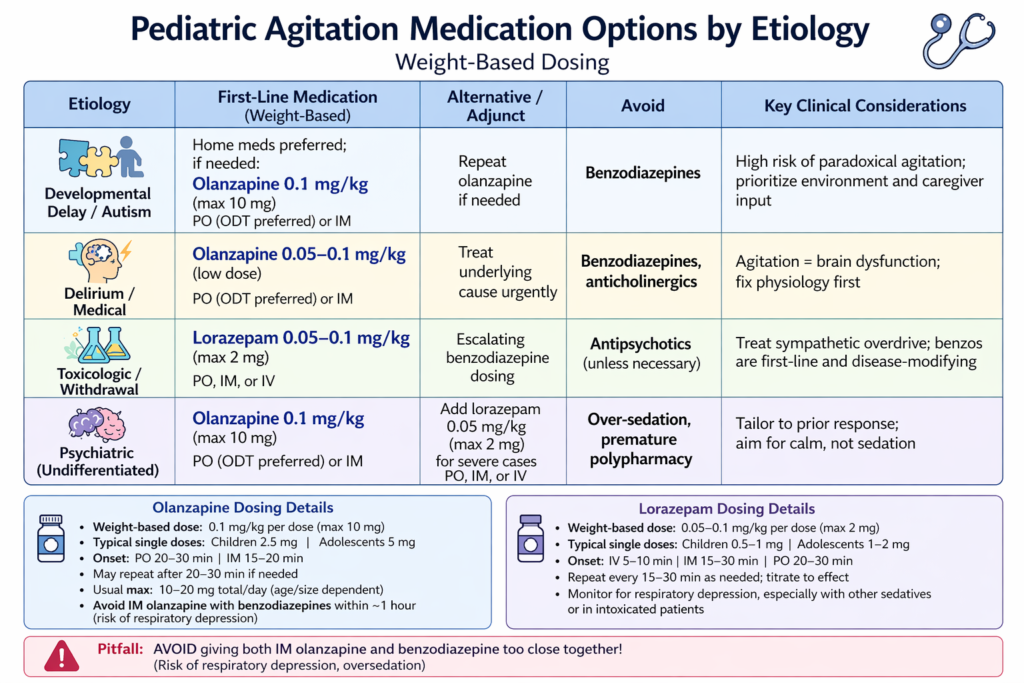
Pharmacologic management of the agitated pediatric patient
When medications are needed, the goal is to calm the patient, not over-sedate them. The ideal medication choice depends on the likely cause of agitation, the urgency of the situation, the patient’s age and co-morbidities, prior medication response, and practical issues such as route and onset of action.
Key principles of medication management of the agitate pediatric patient in the ED:
- Continue verbal de-escalation while planning medications
- Offer oral medication first if feasible
- Avoid trying to place an IV in a severely agitated child
- Know the onset and peak effect of the medication you choose
- Make a safe plan while waiting for the medication to work
For the undifferentiated severely agitated child, a second-generation antipsychotic such as olanzapine is our experts’ go-to agent, with some clinicians using a combination of olanzapine and lorazepam depending on the situation. There are no robust RCTs to guide calming medication choices for pediatric agitation. A truly undifferentiated patient is uncommon; usually, some information about psychiatric history, developmental condition, substance exposure, or prior medication response can be obtained and should guide medication choice.
The oral route is preferred when possible, IM is used when danger is imminent, and IV is rarely needed.
Pearl: Even highly agitated children sometimes accept oral medication if it is presented as a meaningful choice. A child who seems to be heading toward IM treatment may still say, “I’ll take the oral medication.” That moment of choice can preserve dignity and reduce the need for force.
Preventing re-escalation: ongoing environmental management in pediatric agitation
After the patient has settled, the work is not done. The ED remains a high-risk environment for re-escalation. Our experts emphasize that ongoing management of the room and the care process is one of the most important determinants of whether the patient stays calm.
Helpful ongoing strategies include:
- Keep the room low-stimulation
- Limit nonessential staff traffic
- Remove potentially dangerous objects
- Offer food and hydration
- Provide distraction with music, videos, games, or cards
- Use child life experts, caregivers, sitters, or observers constructively
- Revisit what the child says helps them feel safe
- Give regular updates so the patient does not feel forgotten
Other practical examples include: using guided imagery, weighted blankets, sensory tools, headphones, puzzles, and comfort items; allowing a preferred caregiver to remain present; and even maintaining a dedicated “autism closet” or activity closet to improve environmental support.
Revisiting the differential diagnosis in pediatric agitation
Once initial safety is restored, the clinician should return to the underlying cause. The adult EM Cases approach is especially helpful here: after calming medications take effect, clinicians should actively pursue immediate life threats and the diagnosis beneath the agitation.
Reassess for:
- Delirium
- Intoxication or withdrawal
- Trauma
- CNS pathology
- Metabolic derangement
- Infection
- Primary psychiatric illness
- Developmental or sensory contributors
Children with developmental disorders, autism, acute psychosis, intoxication, or trauma-related dysregulation may all look superficially “agitated,” but their optimal management differs. The more clearly the clinician identifies the driver, the safer and more effective the care becomes.
Take-home points for management of pediatric agitation
- Start by classifying pediatric agitation as mild, moderate, or severe, because severity determines the management.
- Anticipate agitation early at triage by identifying prior aggression, trauma, neurodevelopmental conditions, substance use, and other risk factors.
- Prevent escalation with a trauma-informed approach, low-stimulation environment, clear expectations, and attention to the child’s preferences and triggers.
- Use verbal de-escalation early and continuously, with one calm communicator focusing on safety, empathy, and choice.
- Reserve “code white”/emergency security response and physical restraints for imminent danger, never as threats or substitutes for thoughtful care.
- Choose medications based on likely etiology, prior response, and the goal of calming rather than over-sedating.
- Once the patient is calmer, identify and treat the underlying cause of agitation.
References








{kind=link}
{kind=link}